IMAGE OF THE WEEK 2014
IMAGE 11
MEDIASTINAL
TUMOURS: PART 1
|
 |
|
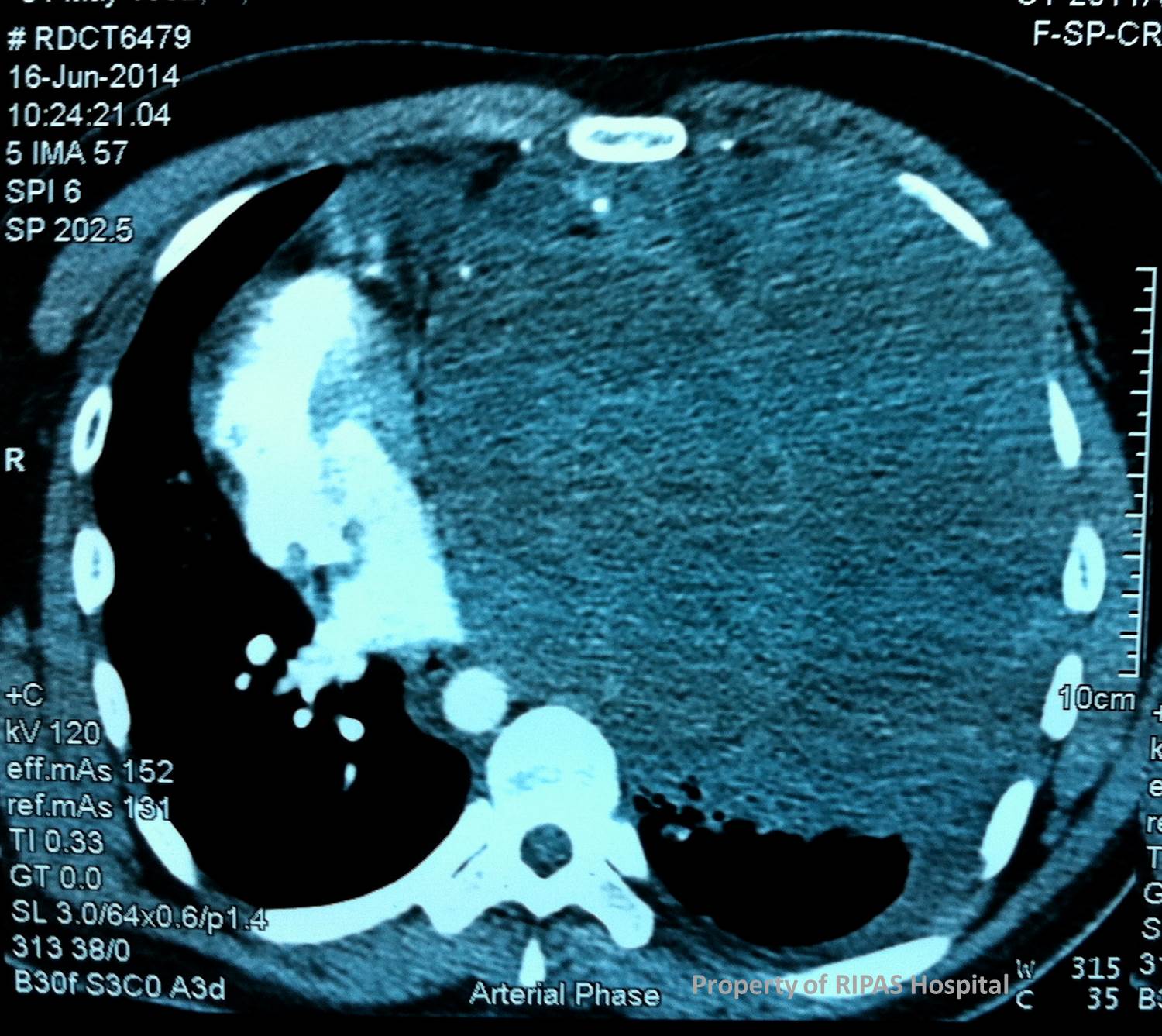
Figure 1: CT thorax showing a large heterogenous
density encapsulated tumour in the left thorax, compressing on the left
lung and pushing the heart and aorta to the right thorax. The
heterogenous density of the tumour indicates area of liquifaction of the
tissue from necrosis post chemotherapy.
(Click on image to
enlarge) |
The mediastinum is anatomically divided into 3 compartments:
Anterosuperior compartment is the space between the sternum and pericardium,
Middle or visceral compartment is bordered by the anterior and posterior
pericardial reflections and finally the posterior compartment which is the
region behind the posterior pericardial reflection which includes the
paravertebral gutter.
Tumours occurring in these mediastinal compartments are
predictable to some degree with some occurring more frequently in certain
compartment then the others as shown in table 1. Tumours occurring in the middle
compartment then to be benign epithelial cyst either of bronchogenic or
pericardial origin while neural tumours are more likely in the posterior
compartment.
|
TUMOURS AND CYSTS BY LOCATION (with decreasing frequency) |
|
ANTERIOR (54%) |
MIDDLE (20%) |
POSTERIOR (26%) |
|
Thymoma |
Enterogenous cyst |
Neurogenic origin |
|
Germ Cell Tumour |
Mesothelial cyst |
Neurenteric cyst |
|
Lymphoma |
Lymphoma |
Lymphoma |
|
Hemangioma |
Thoracic duct cyst |
|
|
Parathyroid adenoma |
Granuloma |
|
|
Thymic cyst |
Hamartoma |
|
|
Lipoma |
|
|
|
Aberrant thyroid |
|
|
|
Lymphangioma |
|
|
Overall the most common tumours are neurogenic (20%), thymomas
(20%), primary cyst (20%), lymphomas (13%), and germ cell tumours (10%). 25-40%
of mediastinal tumours are malignant with majority occurring in the
anterosuperior compartment and patients then to be younger, with ages between 10
– 40 years old. Neurogenic tumours and non-Hodgkin’s lymphomas are the most
common tumours in children.
Majority of patients (60%) with mediastinal tumours usually
present with chest pain, cough and fever. A third of patients are asymptomatic
and is usually a good indicator that the tumour is likely to be benign. Rapid
tumour growth with mediastinal structures compression or invasion is usually a
bad sign indicating malignant tumours as in this case of a large teratoma with
malignant yolk sac tumour component. Patient can also present with
paraneoplastic syndromes such as Cushing’s syndrome, thyrotoxicosis,
hypertension, hypercalcaemia, hypoglycaemia, diarrhea and gynaecomastia.
A chest radiograph will usually showed an enlarged and widened
mediastinum, indicating increased mediastinal tissue density. There may be
calcification. CT scan of the thorax will usually confirmed the presence of a
mediastinal tumour, the presence of chestwall invasion, multiple masses or
extension into the spinal column. MRI is more accurate for vascular involvement
and intracardiac pathology. Echocardiography is useful for patients with middle
compartment tumours to differentiate between intracardiac and pericardial
pathologies. Confirmation of the tumours required tissue biopsies which can be
obtained via radiological route with FNAC or open biopsies via mediastinotomy
incisions.
Germ cell tumours comprise of 15-25% of anterior mediastinal
masses, occurring commonly in children and young adults. Germ cell tumours
include teratomas, teratocarcinomas, seminomas, embryonal cell carcinomas,
choriocarcinomas, and endodermal cell or yolk-sac tumours. This particular case
is one of germ cell tumour with a large matured teratoma and a small component
of yolk cell tumour. About 60% are benign and 40% malignant. Teratomas are
predominantly benign tumours with well differentiated bone, cartilage, nerve or
glandular tissue. Malignant teratomas are differentiated upon histologic
identification of embryonic tissue.
Malignant tumours consist of 40% seminomas and 60% non-seminomas
such as embryonal cell, choriocarcinoma, yolk-sac and teratocarcinoma.
|
|
SEMINOMAS |
NON-SEMINOMAS |
|
AFB/B-HCG |
Rare |
90% |
|
ASSOCIATED SYNDROMES |
None |
Klinfelter’s, trisomy 8, 5q deletion |
|
RADIOSENSITIVITY |
High |
Insensitive |
|
METASTATIC BEHAVIOR |
Remain intrathoracic |
Frequently disseminated |
|
TREATMENT |
Radiation |
Cis-platinum chemotherapy |
|
REMISSION |
Over 80% |
CR in 55-60%, PR in 30-35% |
|
5-YR SURVIVAL |
50-80% |
50-60% |
|
REMISSION |
CR=Complete |
PR=partial |
Images and text contributed by
Mr William Chong, Department of General Surgery,RIPAS Hospital.
All
images are copyrighted and property of RIPAS Hospital.
