IMAGE OF THE WEEK 2014
IMAGE 5
HEART VALVES REPLACEMENT: PART 2 -
MITRAL VALVE STENOSIS
|
 |
|
|
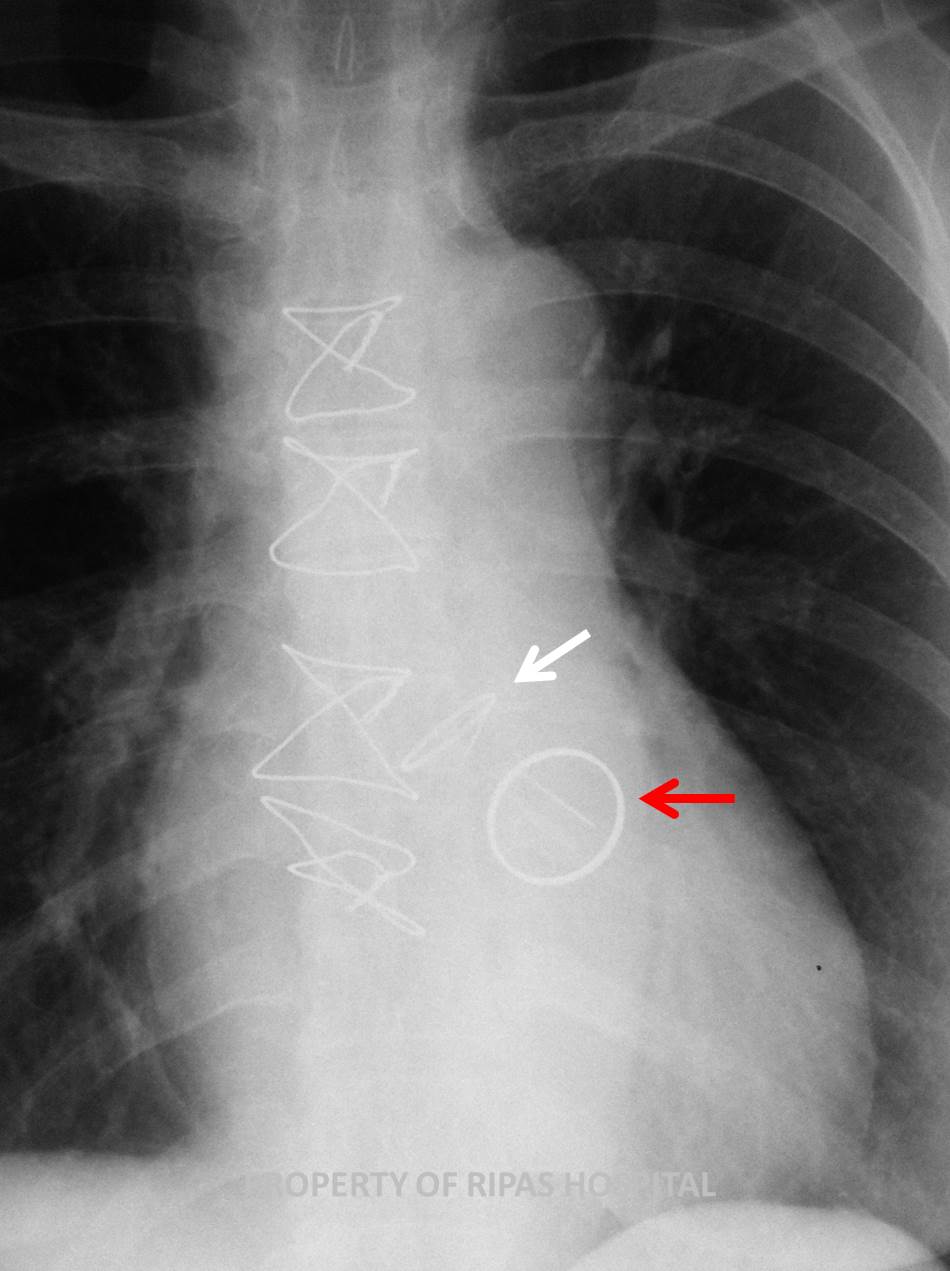
Figure 1: Chest xray of a woman who had undergone
open heart surgery (presence of central sternal wires) with 2 metalic
rings structures inside the heart, one verticle ring and another a
horizontal disc, just above the ring to indicate both mitral and aortic
valves replacement respectively.
(Click on image to
enlarge) |
|
|
|
|
Mitral
stenosis is a condition characterised by a narrowing of the opening of the
mitral valve, resulting in an obstruction of left ventricular inflow tract.
Unlike the aortic valve, the mitral valve consists of 4 structural components
(Annulus, chordae, papillary muscles and leaflets) which can be individually
affected causing stenosis but in most cases, are a combination of abnormalities
of 2 or more structures. The aetiologies of mitral valve stenosis can be classified into
2 groups as shown in the table below:
Table
1: Aetiologies of aortic stenosis
|
Neonate/Infant/Children |
Acquired |
|
Congenital mitral stenosis |
Rheumatic mitral stenosis |
|
Cor Triatriatum |
Infective endocarditis with
large vegetation |
|
|
non-rheumatic mitral
annular calcification |
|
|
Rheumatic heart disease |
|
|
Ball valve thrombus |
|
|
malignnant carcinoid disease |
|
|
SLE |
|
|
Rheumatoid arthritis |
|
|
mucopolysaccharidosis of the Hunter-Hurler phenotype |
|
|
Fabry disease |
|
|
Whipple disease |
|
|
Methysergide therapy |
The
natural history of acquired aortic stenosis is one of progressive narrowing with
a latent period of 10-20 years in which the patient remains asymptomatic. Once
symptoms developed which consists of a triad of chest pain, heart failure and
syncope, indicating moderate-to-severe aortic stenosis, the patient’s condition
usually deteriorate rapidly and death can occurred within 3 years if left
untreated, with a mortality of approximately 25% at 1 year and 50% at 2 years.
Severe aortic stenosis is defined as an aortic valve orifice area of less than
1.2cm2/M2 or an LV to Ao gradient greater than 50mmHg.
Clinical signs of aortic stenosis include:
·
Pulsus
alternans due to presence of left ventricular systolic dysfunction
·
Ejection
click due to stiffness of aortic leaflets due to calcification which snaps open
when force by the jet of blood passing through the aortic valve orifice
·
Ejection
systolic murmur
·
Signs of
LV hypertrophy includes ECG changes of large amplitude R wave, LBBB or RBBB, ST
depression or T wave invertion.
·
There
may be signs suggestive of coronary artery disease
Aortic
Valve Replacement
Indications for surgery is dependent on the severity of the aortic stenosis. For
symptomatic patients, the aortic stenosis is usually moderate to severe and will
need prompt aortic valve replacement to avoid sudden death or rapid
deterioration. For mild aortic valve stenosis, operation is not urgent but
patients should be regularly followed up to assess condition as disease
progresses.
Preoperative preparations
·
Blood
investigations: FBC, Renal panel, LFTs, coagulation screen, cross match.
·
ECG,
Echocardiography to assess severity of stenosis and LV function, TOE for better
assessment particularly of root and sinotubular dimension as well as in
endocarditis for root abscess.
·
Coronary
angiogram to exclude coronary artery disease if indicated.
·
Dental
check -up to repair or extract decayed tooth and resolve all dental caries.
There
are several choices of replacement valves and are indicated based on age (Table
2). The main categories are divided into 2 groups: mechanical and tissue valves.
Table
2: Choice of aortic valve replacement
|
Age |
Valve Choice |
Brand available |
|
< 55years |
Aortic allograft or pulmonary allograft (homograft) |
|
|
55-75 years |
Mechanical valves |
St. Judes, Carbomedics, Metronic Hall, ATS Open Pivot
valves and On-X and Conform-X valves. |
|
>75 years |
Bioprosthesis valves, stented or stentless |
Carpentier-Edwards Porcine tissue valve, Carpentier-Edwards
bovine perimont valves, Hancock aortic bioprosthesis. |
As
shown in the chest radiograph Figure 1 and Figure 2 (annotated), this patient
has bivalve replacement using both mechanical St Judes Mechanincal valves as
indicated by the opaque sewing ring and 2 parallel hinge points where the carbon
leaflets are attached.
|
 |
|
Figure 2: Annotated image of Figure 1 with white
arrow pointing at the aortic valve which sits horizontally to the base
of the heart while the mitral valve appears as a ring and sits vertical
to the base of the heart (red arrow).
(Click on image to
enlarge) |
|
|
Survival after AVR
·
Early
(hospital) mortality ranges from 3-6%
·
5-yr
survival – 75%
·
10-yr
survival – 60%
·
15-yr
survival – 40%
Predictors of Survival
·
Age –
Advanced age significant predictor of survival and cardiac events
·
Pre-op
LV function
Post
operative management
·
Maintain
INR of 2.5 – 3.5 using Warfarin for mechanical valves,
·
For
bioprosthesis, depending on units protocol, may need Warfarin for the first 3
months to allow for the sewing ring to endothelise before stopping Warfarin
·
Cover
with antibiotic Amoxycillin 1.2 g for invasive procedures where breach of
epithelium may occur.
For more information
on:
Aortic stenosis,
please visit this link
http://emedicine.medscape.com/article/150638-overview#a0156
Prosthetic heart
valve, please visit this link
http://emedicine.medscape.com/article/780702-overview
Images and text contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
and
Dr Chong Chee Fui, Department of Surgery, RIPAS
Hospital
All
images are copyrighted and property of RIPAS Hospital.
