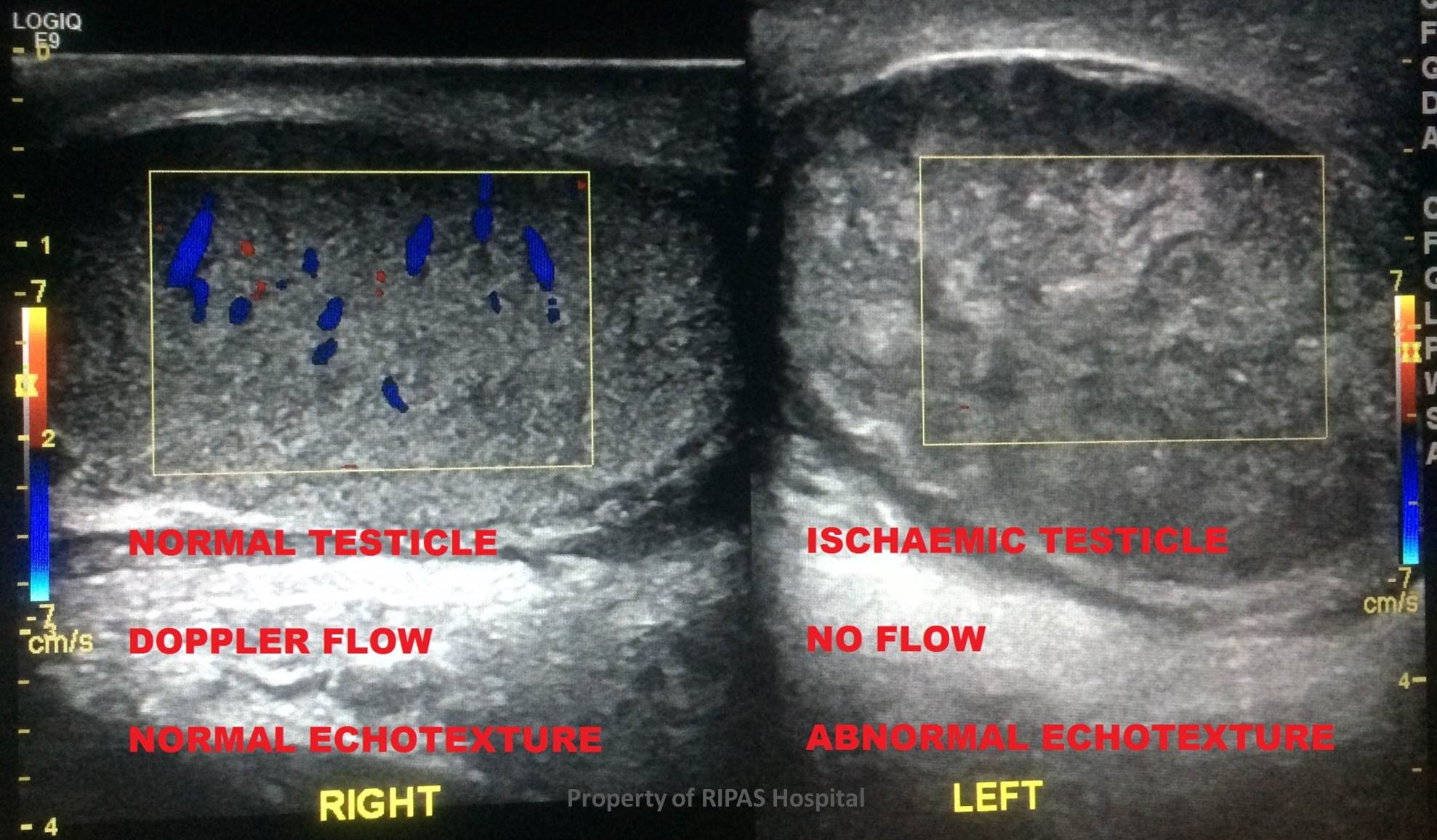
Figure 1: Longitudinal ultrasound colour Doppler of a normal testicle (labelled “RIGHT”) and an ischaemic testicle (labelled “LEFT”)(Click on image to enlarge)
IMAGE OF THE WEEK 2014
IMAGE 15
TESTICULAR TORSION WITH ISCHAEMIC TESTICLE
|
|
|
|
Figure 1: Longitudinal ultrasound colour Doppler of a normal testicle (labelled “RIGHT”) and an ischaemic testicle (labelled “LEFT”)(Click on image to enlarge) |
|
Ischaemia of the testis is one of the most common urological emergencies and is categorised by obstruction of the pre-testicular vasculature leading to ischaemic injury. The three vessels supplying the testes; the testicular, cremasteric and deferential arteries, pass within the spermatic cord through the inguinal canal to pierce the testicle in the posterior of the tunica albuginea.
Testicular torsion occurs when there is twisting of the spermatic cord. Ischaemia of the testicles occur as blood is obstructed from reaching the testis through the occluded spermatic cord. Pre-dispositions to testicular torsion include larger testicle size (physiological or pathological – tumour of the testis) and the congenital condition known as the “bell-clapper deformity” where the testis fails to securely anchor to the scrotum allowing it to move and rotate freely.
The patient typically presents with an acutely painful and often swollen testicle.
Testicular torsion remains a largely clinical diagnosis, with supportive ultrasound imaging of the scrotum.
Colour Doppler ultrasonography (CDS), alongside accurate patient history and careful examination, is the current gold standard for diagnosis of testicular ischaemia.
In the normal testes CDS shows centripetal, centrifugal and occasionally trans-testicular arteries within the testicular parenchyma (Figure 1&2). In the case of an acute ischaemic testis, CDS demonstrates a lack of flow through the intrinsic vasculature of the testes. Ischaemic testes also exhibit altered echotexture; displaying heterogenous and hypoechoic parenchyma (Figure 1 & 2).
|
|
|
|
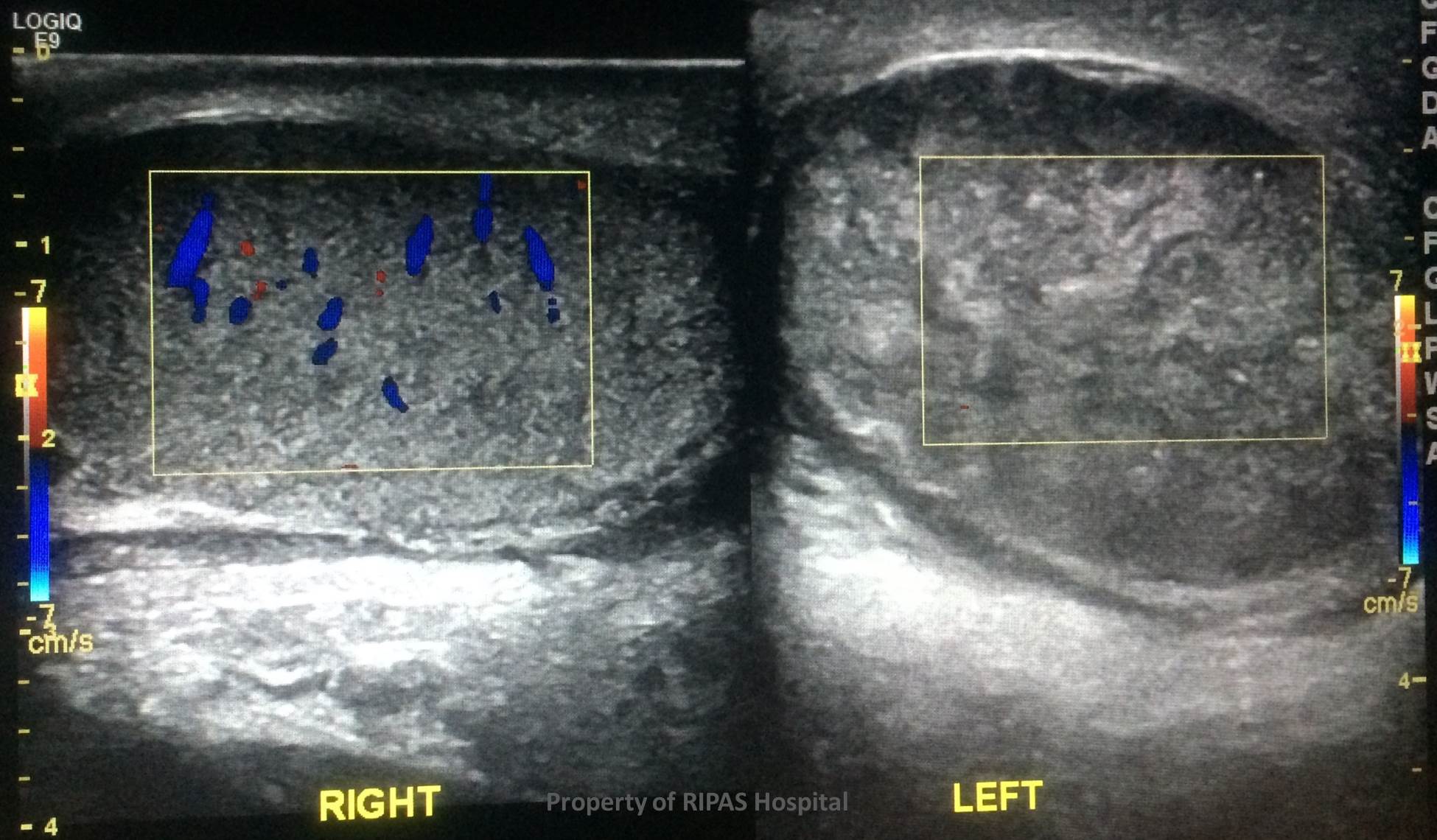
Figure 2: Longitudinal ultrasound colour Doppler indicating the absence of Doppler flow and the abnormal coarse echotexture of the ischaemic testicle (left) in comparison to the normal right testicle (Click on image to enlarge) |
Treatment is with immediate surgical repair and untwisting of spermatic cord is required in testicular torsion to salvage testis. A significant number of torsions are missed with surgical exploration resulting in an orchidectomy for an infarcted/necrotic testicle (Figure 3).
|
|
|
Figure 3: Intra-operative image of ischaemic testicle with twisted spermatic cord. (Click on image to enlarge) |
Images and text contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital.
Text contributed by
Matthew Hon and Samuel Jackson, School of Medicine, University of Queensland.
All images are copyrighted and property of RIPAS Hospital.
![]()