IMAGE OF THE WEEK 2014
IMAGE 10
INTUSSUSCEPTION
|
 |
|
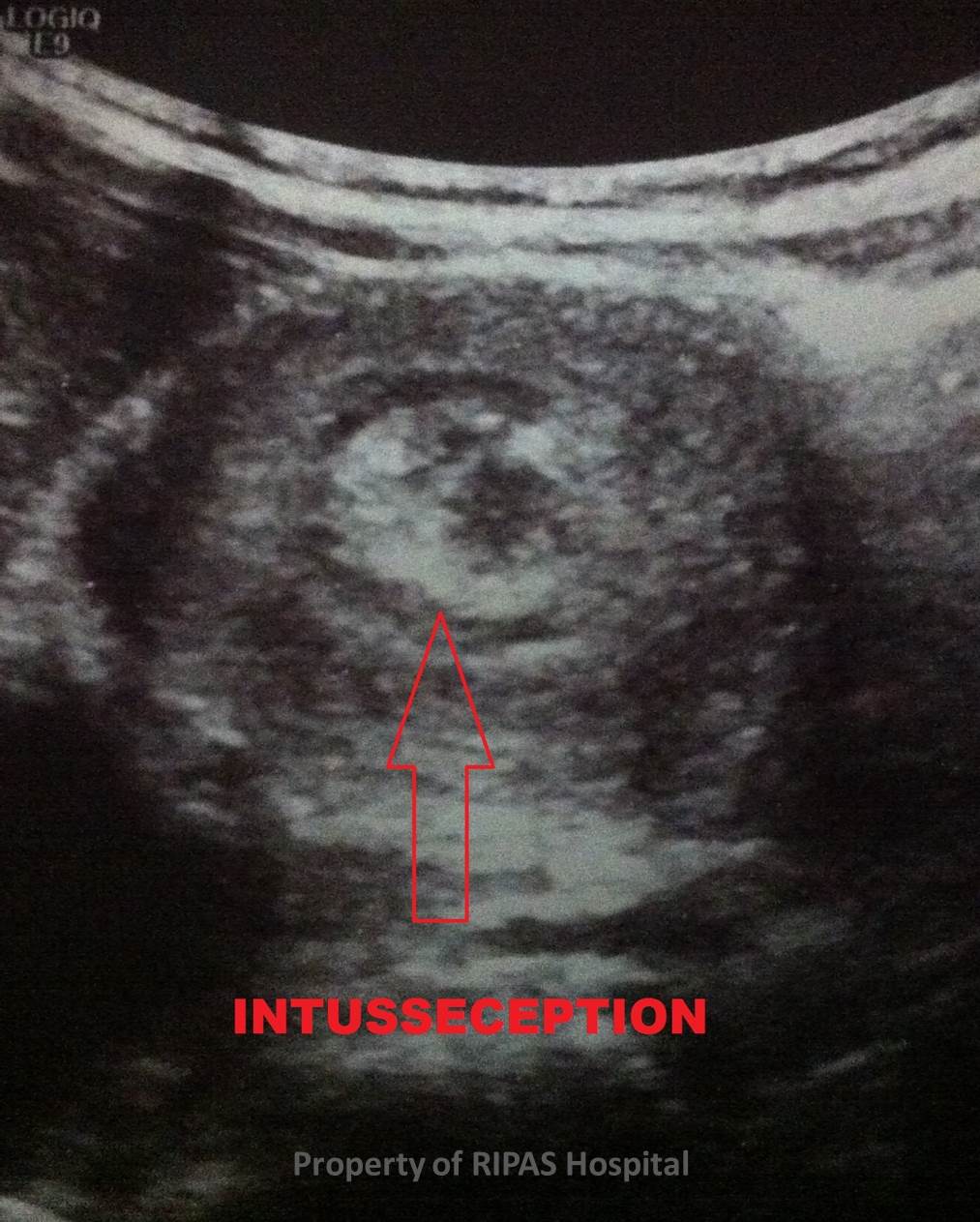
Figure 1a: Abdominal ultrasound showing presence of
a lymph node acting as a lead point resulting in intussusception of the
small bowel, as indicated by a target or doughnut sign on ultrasound of
the affected bowel segment.
(Click on image to
enlarge) |
Intussusception is a clinical condition caused by the
invagination of a segment of small bowel into the adjoining bowel lumen,
resulting in bowel obstruction. It is a common cause of intestinal obstruction
in children aged between 6 months to 2 years. The incidence then to be higher
in the male gender than female with a ratio of 3:1.
The higher incidence of intussusception in children above 6 years
of age has been thought to be linked to the starting of solid feeding in a
child.
Clinical signs and symptoms of intussusception in a child
includes the following:
·
Vomiting
which is non-bilious initially but becomes bilious when bowel obstruction sets
in,
·
Abdominal
pain is colicky and severe, which cannot be settle with normal parental
measures,
·
Passage of
blood mixed with mucus, typically described as red current jelly generally
indicate a more advance stage of intussusception due to sloughed mucosa from
ischaemia, diarrhoea may be an early sign of intussusception,
-
Palpable
abdominal mass in a thin child, which is best detected between spasms of
colic, when the child is quiet and the typical or hallmark physical findings
in intussusception is a right hypochondrium sausage-shaped mass and
emptiness in the right lower quadrant commonly known as the Dance sign.
·
Abdominal
distension in the presence of bowel obstruction.
Imaging is the main stay of diagnosis of intussusception which
includes the following:
·
Plain
abdominal x-ray may reveals signs suggestive of intussusception in 60% of cases,
·
Ultrasonography is the gold standards as shown in the above images, which
includes typical donut shaped mass or target sign (Figure 1 & 2 ) and
pseudokidney signs,
·
Contrast
enema is the traditional and most reliable way to make the diagnosis of
intussusception in children (Figure 3)
|
 |
|
Figure 1b: Magnified image from Figure 1a showing
the intussusception of the small bowel.
(Click on image to
enlarge) |
|
 |
|
Figure 2: Abdominal ultrasound showing magnified
image from Figure 1a with an image of a dognut insert, reflecting the
similarity of the ultrasound image of the bowel intussusception.
(Click on image to
enlarge) |
|
 |
|
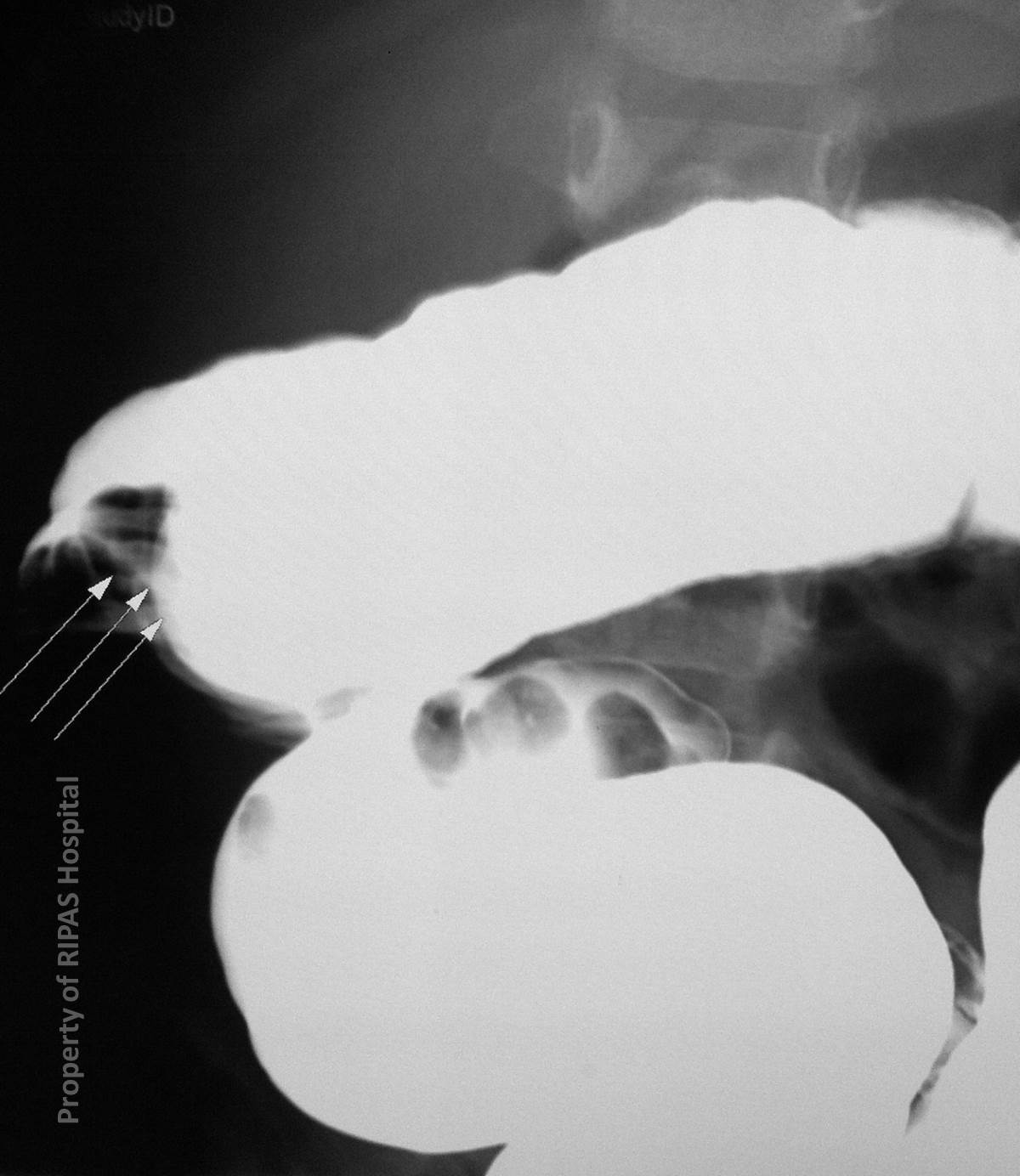
Figure 3: Small and large bowel enema showing the
intussusception (three white arrows). The enema can be used to reduce
the intussusception.
(Click on image to
enlarge) |
The initial management of intussusception is resuscitation by
ensuring rehydration of the child or patient with iv fluids. Non-operative
radiological reduction can be performed using therapeutic enemas which can by
hydrostatic with barium or water soluble contrast or pneumatic with air
insufflation.
Surgical reduction is reserve for failed medical management and
is traditional performed through a right paraumbilical incision. The
intussusception is delivered into the wound and manual reduction performed. If
manual reduction cannot be performed or in the presence of perforation, a
segmental resection of the affected segment including the lead point should be
carried out with end to end anastomosis. This procedure can also be carried out
successfully using laparoscopic approach.
Images contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital.
Text
contributed by
Mr William Chong, Department of General Surgery,RIPAS Hospital.
All
images are copyrighted and property of RIPAS Hospital.
