IMAGE OF THE WEEK 2015
IMAGE 02 - 19 February 2015
NEONATAL DIAPHRAGMATIC HERNIA
|
 |
 |
|
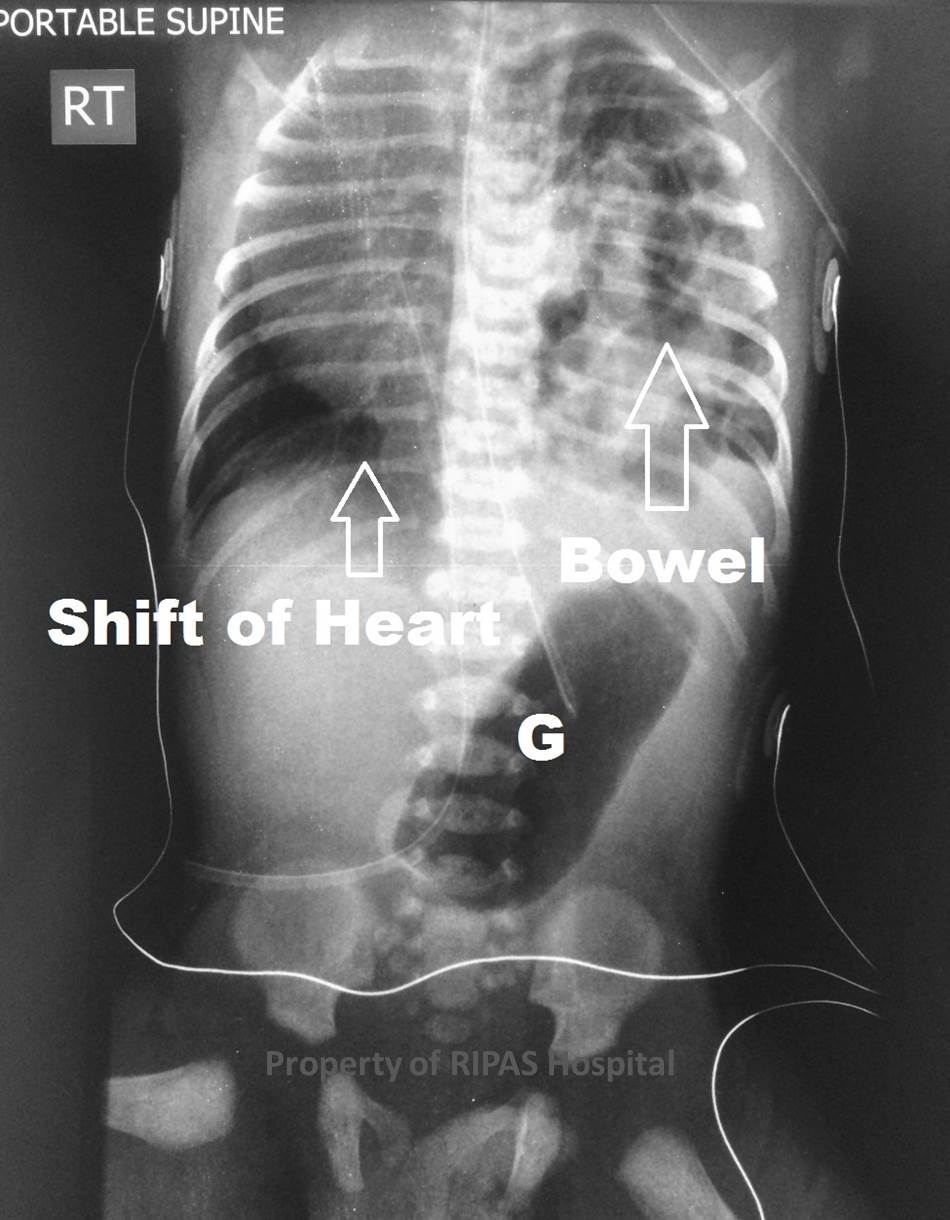
Figure 1: PA x-ray of a neonate with a congenital diaphragmatic hernia. (Click on image to
enlarge) |
Figure 2: Annotated image of Figure 1, showing displacement of a large
portion of small bowel in the left hemithorax with displacement of the
heart and mediastinal structures into the right hemithorax. the stomach
remains in the abdomen. (Click on image to
enlarge)
|
Figure 1&2: Posterior-anterior X ray of a neonate with a congenital
diaphragmatic hernia. A large portion of small bowel can be seen in the left
hemithorax. The stomach remains within the abdomen.The heart and mediastinal
structures are displaced to into the right hemithorax.
Congenital Diaphragmatic Hernia (CDH) is a birth defect of the diaphragm that
allows the contents of the abdomen to enter the thoracic cavity. CDH is a rare
congenital condition affecting about 1 in 3000 live births. The mortality rate
varies between 40 and 60% with the prognosis dependent on several factors
including; the size of the hernia, the organs involved, and other birth defects.
There is also evidence around 30% of foetuses with CDH are electively terminated
most often due to multiple congenital complications. The two major causes of
death associated with CDH are pulmonary hypoplasia and pulmonary hypertension,
both contributing to the severe respiratory distress of the infant.
CDH is divided into four categories based on the location and congenital defect
underlying the herniation. The most common form is Bochdalek hernia which occurs
in the posterolateral portion of the diaphragm and constitutes approximately 95%
of all CDHs (See figure 1). Bochaleck’s hernia may be due to an innate defect in
the diaphragm or caused by interruption of pleuroperitoneal canal fusion by
thoracic loops of bowel or other abdominal organs which then become trapped. The
remaining 5% of CDHs are classified as Morgani hernia (an anterior defect),
diaphragmatic eventration or as a central tendon defect. Regardless of the cause
40 – 50% of CDHs are associated with at least one other malformation; most often
a cardiac, pulmonary or neural tube defect.
The most common presentation of CDH is respiratory distress which can present as
cyanosis, intercostal retractions or grunting respirations. Other common
presentations of CDH include a scaphoid abdomen, a barrel-shaped chest, and a
shift in the position of heart sounds. Other dysmorphisms closely associated
with CDH include craniofacial and extremity abnormalities.
X-ray and ultrasound are often used to confirm a diagnosis of CDH. In a
Bochdalek hernia the X ray will demonstrate a substantial portion of bowel in
one hemithorax (on the left in 85% of cases) and opacification of the diaphragm
on the affected side (See figure 1). The inclusion of the stomach, liver and
spleen in the herniation is variable. There are often signs of pulmonary
hypoplasia on the side of the hernia. Routine perinatal ultrasound will show
cardiomediastinal shift, elevated stomach or portal veins and a reduction of
bowel loops in the abdomen.
The first priority in management is to address the respiratory failure of the
neonate. An oro-gastric tube is immediately inserted and the neonate is
intubated. In the management of some cases, extracorporeal membrane oxygenation
(ECMO) is used to bypass the infant’s lungs and supply oxygenated blood so
alleviating pulmonary hypertension. Medications, such as vasodilating agents,
vasoactive agents and opioid analgesics are usually administered to regulate
blood pressure, circulating volume, and pulmonary distress.
In the repair of the hernia, surgical intervention is required. The abdomen is
opened and the diaphragm is patched with either a synthetic patch or a sliced
section of the abdominal muscle. Abdominal organs displaced in the chest are
corrected.
Images and text contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital.
Text
contributed by
Matthew
Hon and Samuel Jackson, School of Medicine, University of Queensland.
All
images are copyrighted and property of RIPAS Hospital.
