IMAGE OF THE WEEK 2015
IMAGE 04 - 27 JULY 2015
GIGANTIC GOITRE
|
 |
 |
|
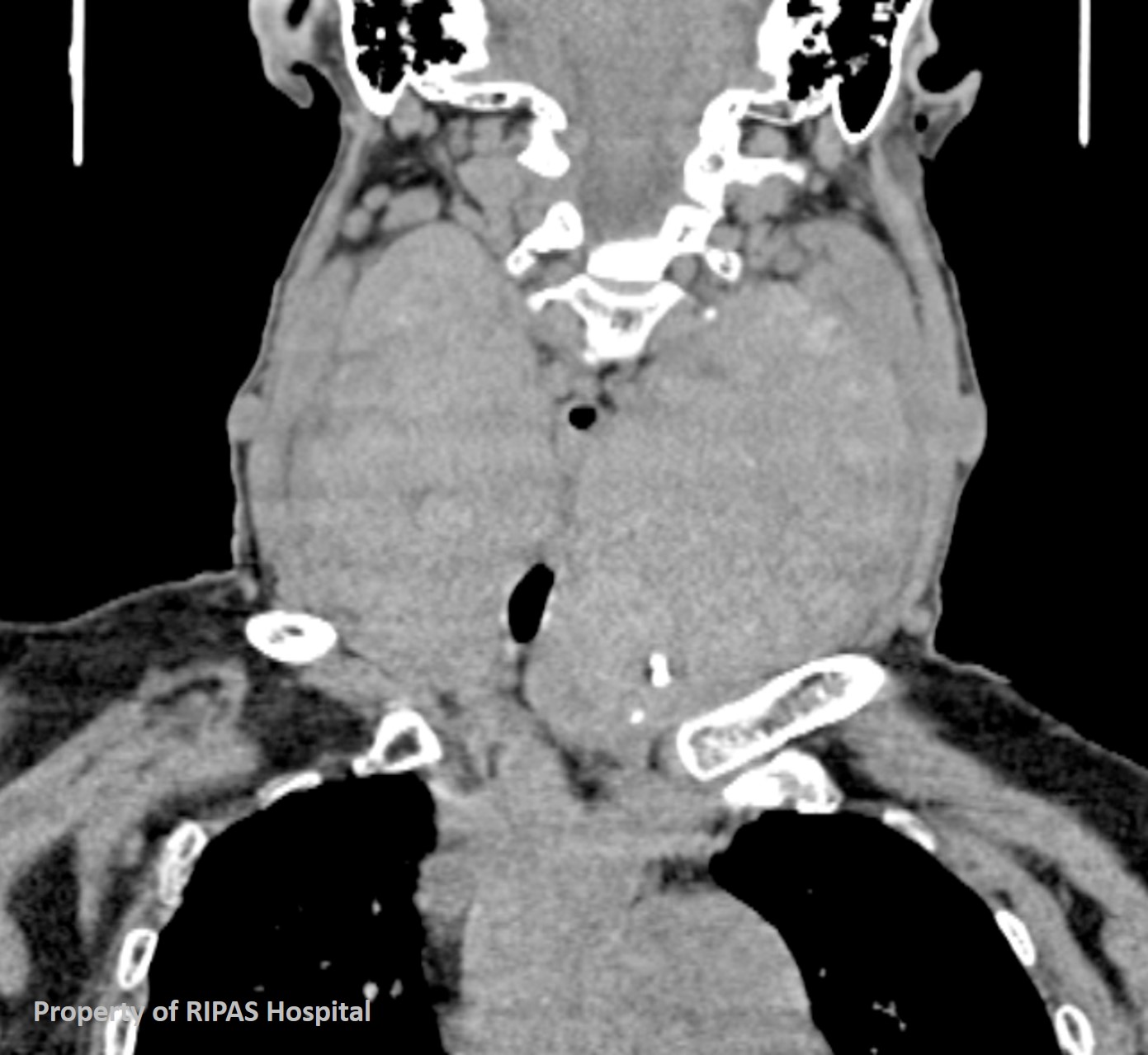
Figure 1: CT coronal section through the neck showing the presence of a
large thyroid mass involving both lobes and compressing on the trachea.
there is a also intrathoracic involvement with substernal extension. (Click on image to
enlarge) |
Figure 2: CT transverse section of the same patient showing the enlarged
thyroid gland with narrowing of the tracheal from external compression
and a calcified structure in the substance of the left thyroid lobe. (Click on image to
enlarge)
|
A goitre is an enlarged thyroid gland (Figure 1). Worldwide, iodine deficiency
represents the most common cause. The vast majority of goitres are benign.
Clinically, goitres can be euthyroid, hyperthyroid or hypothyroid.
Thyroid cancers can also develop from goitres, which occur due to reduced
thyroid hormone production secondary to iodine deficiency, immunological or
biochemical causes.
Hyperthyroidism indicates an overactive thyroid gland leading to the release of
excessive circulating thyroid hormones. The most common cause is Graves disease.
Hypothyroidism reflects lowered thyroid gland activity, and iodine deficiency
remains the most common cause worldwide. However, Hashimoto’s thyroiditis is the
most common cause in the first world. Management for hyperthyroidism typically
includes the antithyroid drugs carbimazole, methimazole and/or propylthiouracil
or radioiodine. Subtotal thyroidectomies can also be considered, although risks
include hypoparathyroidism and laryngeal nerve palsies. Hypothyroidism is
generally treated with thyroxine replacement.
Generally, the diagnosis for hyperthyroid/hypothyroid conditions involve TSH
assays and circulating thyroid hormone (T3 and T4) levels. Additional tests
include; TSH receptor antibody levels, thyroglobulin and thyroid peroxidase (TPO)
autoantibody levels for Graves disease and Hashimoto’s disease.
|
 |
|
|
Figure 3: CT saggital section of the same
patient at the level of the neck showing a grossly enlarge gigantic
thyroid mass, occupying the entire neck and extending into the chest.
The neck is clinically enlarged with a large mass. (Click on image to
enlarge) |
|
An examination of the thyroid gland and cervical lymph nodes should be part of
the clinical assessment. Any palpable thyroid lump should be investigated with
fine-needle aspiration cytology (FNAC) to rule out malignancy.
Ultrasound is most useful for distinguishing solitary nodules from multinodular
nodules and to determine tumour composition. Increased vascularity, echogenicity
and calcifications on ultrasound are potential indicators of malignancy.
Ultrasound is also used to evaluate the cervical lymph nodes. It is also used to
aid image guided FNAC of nodules.
Radionuclide imaging is the most effective imaging modality for the
investigation of thyroid nodules. ‘Cold’ nodules do not uptake radioisotopes,
and are more likely to be malignant. ‘Hot’ nodules uptake radioisotopes, and are
less likely to be malignant. However, there are no specific features that can
indicate or rule out malignancy definitively. Its availability, cost and study
time may be prohibitive.
CT or MRI is indicated when clinical findings suggest invasion beyond the
thyroid capsule, suggested by voice hoarseness, stridor, dysphagia, vocal cord
palsies or lesional fixation (Figure 2).
CT is also used to evaluate nodal involvement and retrosternal extension for
surgical planning (Figure 1 and 3). Generally, non-contrast imaging is preferred
as iodinised contrast uptake can reduce thyroid radioiodine uptake and thus
ablation.
References
1.
Palazzo, Fausto. "Goitre and thyroid cancer." Medicine 37.8
(2009): 436-439.
2.
Sheppard, Michael C. "Goitre and thyroid cancer." Medicine 33.11
(2005): 35-37.
3.
Campbell, Kirsten, and Matthew Doogue. "Evaluating and managing patients
with thyrotoxicosis." Australian family physician 41.8 (2012): 564.
4.
Hughes, Kiernan, and Creswell Eastman. "Goitre: Causes, investigation and
management." Australian family physician 41.8 (2012): 572.
5.
So, Michelle, Richard J MacIsaac, and Mathis Grossmann. "Hypothyroidism,
investigation and management." Australian family physician 41.8 (2012):
556.
6.
Weetman, Anthony P. “Thyrotoxicosis.” Medicine 37.8 (2009):
430-435
7.
Cox, Marcela. “Thyroid Imaging and biopsy.” Australian Doctor 33
(2005)
8.
Aiken, Ashley H. "Imaging of thyroid cancer." Seminars in Ultrasound,
CT and MRI 30 Apr. 2012: 138-149.
Images and text contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital and
Christopher Yii Bong, medical student.
All
images are copyrighted and property of RIPAS Hospital.
