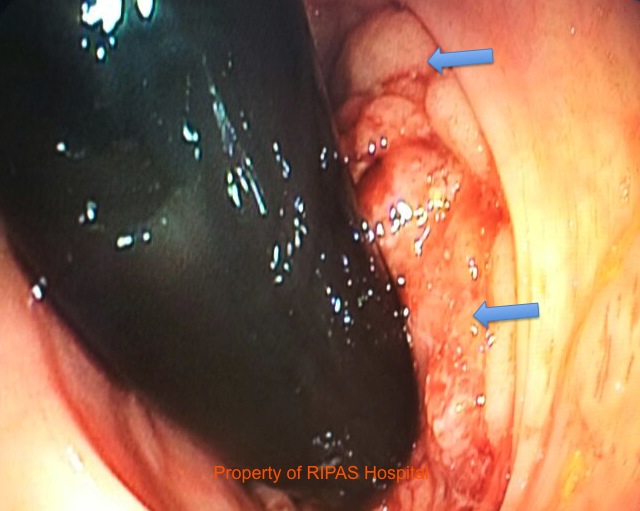
Figure 1: Flexible colonoscopy assessement of a fleshy lobulated rectal mucosal tumour with broad base protruding into the lumen (Blue arrows).
(Click on image to enlarge)
IMAGE OF THE WEEK 2013
WEEK 1
rectal carcinoma
|
|
|
|
Figure 1: Flexible colonoscopy assessement of a fleshy lobulated rectal mucosal tumour with broad base protruding into the lumen (Blue arrows). (Click on image to enlarge) |
In Brunei Darussalam, cancer is the top leading cause of deaths, at a rate of 65.1/100,000 population in 2011, with colorectal malignancy coming second after lung cancer.1 The age-standardised incidence rate for colorectal cancer in Brunei Darussalam in 2008 was reported to be about 38.3/100,000 population, which is the second highest after Thailand, among the 10 ASEAN countries.2
Of all the colorectal carcinoma, rectal carcinoma (Figure1, 2a & b) makes up about 27% of the colorectal carcinoma and the most common histological type is adenocarcinoma. Rectal carcinoma usually evolved in the beginning as a precancerous polyp which over many years developed into invasive carcinoma. The actual aetiological cause is unclear but risk factors associated with rectal carcinoma development includes increasing age, smoking, positive personal or family history of colorectal carcinoma or polyps, high fat (animal source) diet and diet containing preserved food containing nitrosamines.
|
|
|
|
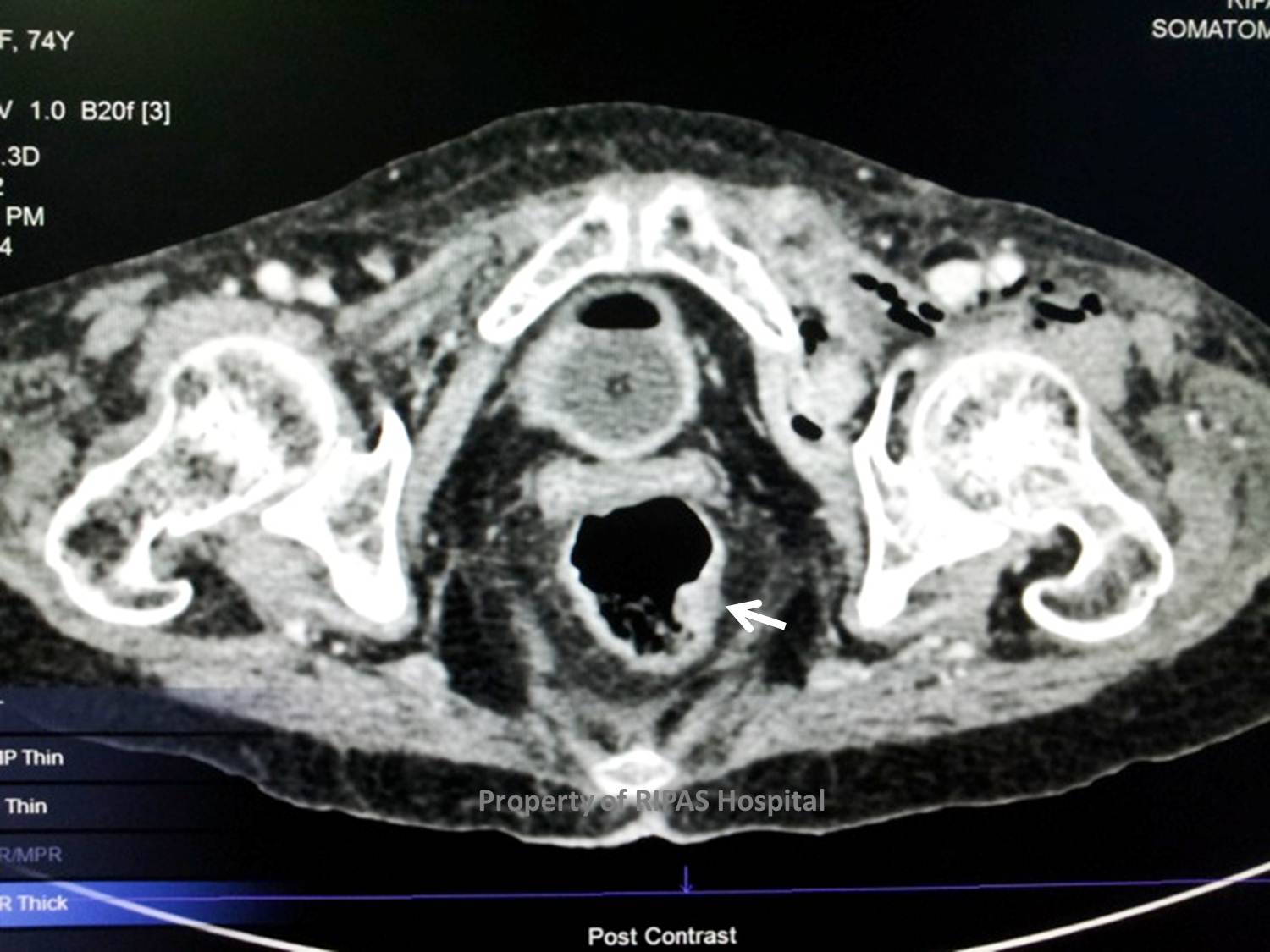
Figure 2a: CT pelvis at the hip joint level, showing a widely patent rectum with a small mucosal lesion protruding into the lumen (white arrow). (Click on image to enlarge) |
Figure 2b: MRI scan of the same patient at a level lower than Figure 2a showing a thickened mucosal lesion posteriorly occupying almost 2/3 of the rectal lumen (white arrow). (Click on image to enlarge) |
Signs and symptoms of rectal carcinoma as in the case presented, will include:
· Fresh PR bleeding, mixed with stool (most common cause of PR bleeding is haemorrhoids),
· Prolonged and recurrent PR bleeding, leading to anaemia, fatigue etc,
· Change of bowel habits – constipation, frequent motion, tinismus (sensation of incomplete emptying of bowel),
· Weight loss
Investigations begin with a thorough history and physical examination, which includes a digital rectal examination. Stool samples should be examined for fecal occult blood, using in 3 separate specimens. Blood investigations should include a FBC (to exclude anaemia), liver function tests and tumour markers such as carcinoembryonic antigen (CEA). This should then be followed by a sigmoidoscopy (flexible or rigid) examination with biopsies if mucosal lesions are seen or colonoscopy (Figure 1).
Radiological investigations should include a double-contrast barium enema if CT scan is not easily available. Double-contrast barium enema has a sensitivity of about 80-95% but it should be preceded by a flexible sigmoidoscopy and it has low perforation rate (1/25,000). However, CT scan is the choice of primary investigation now which should be a staging CT, including chest, abdomen and pelvis. CT scans has a sensitivity of 50% for local invasion and an accuracy rates of 53-94% for depth of penetration and 54-70% for lymph node metastases. MRI is more accurate than CT scan and can also be performed for a more closer assessment of mural invasion or invasion to surrounding organs.(Figure 2b). MRI accuracy varies from 66-92% for depth of penetration and 60-90% for lymph node metastases, with a higher sensitivity (91%) and specificity (100%) compared to CT scan (82%) and (69%) respectively, in detecting local recurrence.
Prognosis of rectal carcinoma is dependant on the stage of the tumour. Staging of rectal carcinoma is carried out according to the TNM stage or modified Dukes stage as shown below.
|
TNM Stage |
Modified Dukes Stage |
Description |
5-yr Survival rate, % |
|
T1N0M0 |
A |
Limited to submucosa |
83 |
|
T2N0M0 |
B1 |
Limited to muscularis propria |
70 |
|
T3N0M0 |
B2 |
Transmural extension |
30-70 |
|
T2N1M0 |
C1 |
T2, enlarged mesenteric nodes |
30 |
|
T3N1M0 |
C2 |
T3, enlarged mesenteric nodes |
10-30 |
|
T4 |
C2 |
Invasion of adjacent organs |
10-30 |
|
Any T, M1 |
D |
Distant metastases present |
10 |
Surgical management of rectal carcinoma is either by anterior resection or total mesorectal excision. Total mesorectal excision is the preferred surgical treatment modality of early rectal carcinoma as it addresses early treatment concerns regarding adequate local control while performing an anterior resection. It is essentially a low anterior resection for tumours of the middle and lower third of the rectum with the complete removal of the mesorectum up to the level of the levators. For extremely low rectal tumour, abdomino perineal excision of the rectum can be performed. Circumferential resection margin positivity rate is about 5% or less for low anterior resection with total mesorectal excision of the rectum, whereas the positivity rate with abdominoperineal excision of the rectum is about 10-25%.
1. Brunei Darussalam M. Health Information Booklet (HIB) 2011 [Internet]. 2013 Jan. Available from: http://www.moh.gov.bn/satisticshealthguidelines/indicators.htm
2. Kimman M, Norman R, Jan S, Kingston D, Woodward M. The burden of cancer in member countries of the Association of Southeast Asian Nations (ASEAN). Asian Pac. J. Cancer Prev. 2012;13(2):411–20.
Images and text contributed and prepared by
Mr Chee Fui Chong, Department of Surgery.
All images are copyrighted and property of RIPAS Hospital.
![]()