IMAGE OF THE WEEK 2013
WEEK 10
LUNG
BIOPSY TECHNIQUES
|
 |
 |
|
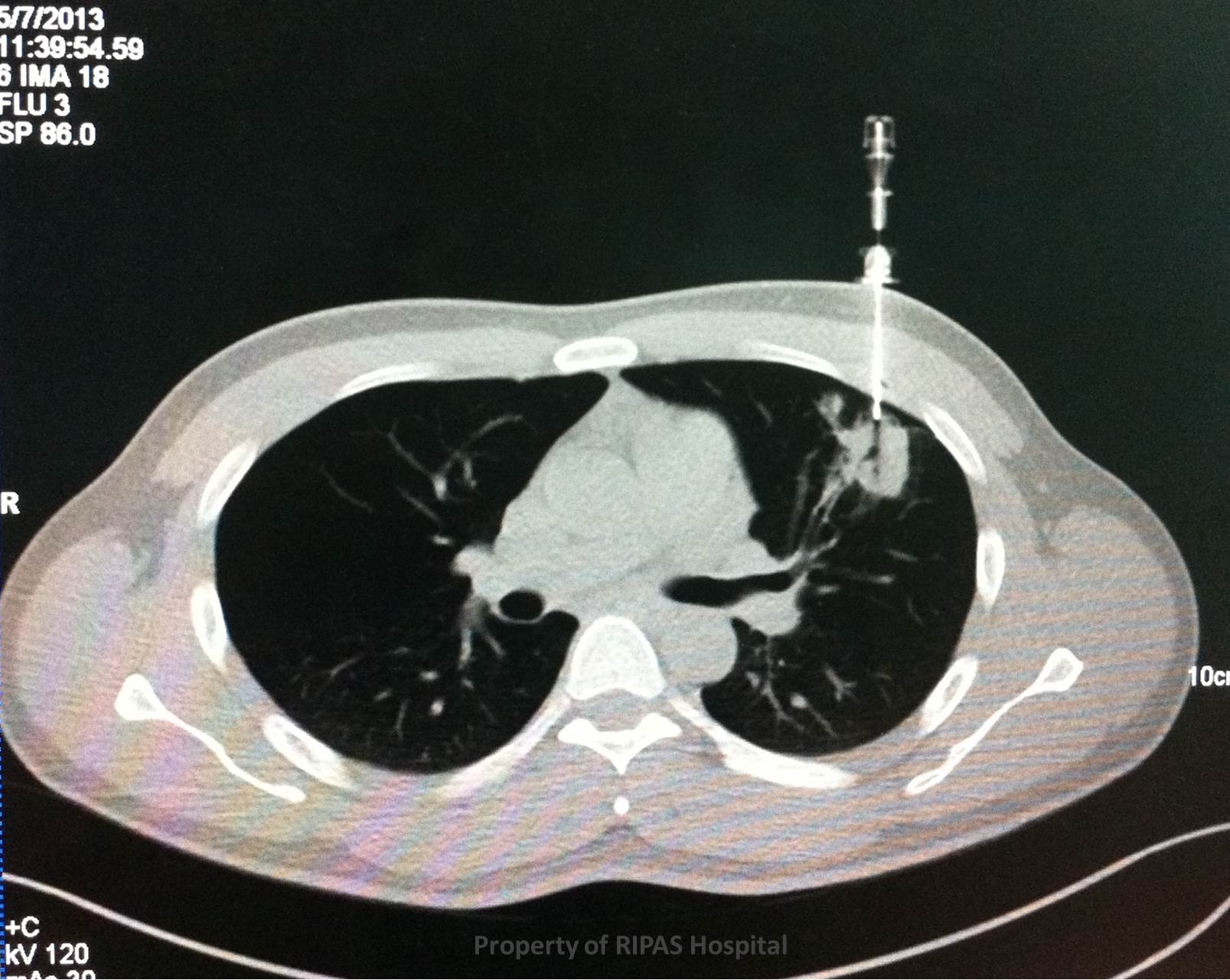
Figure 1a: CT chest showing a left upper lobe lung
nodule with a co-axial needle inserted into the nodule for fine needle
aspiration cytology (FNAC).
(Click on image to
enlarge) |
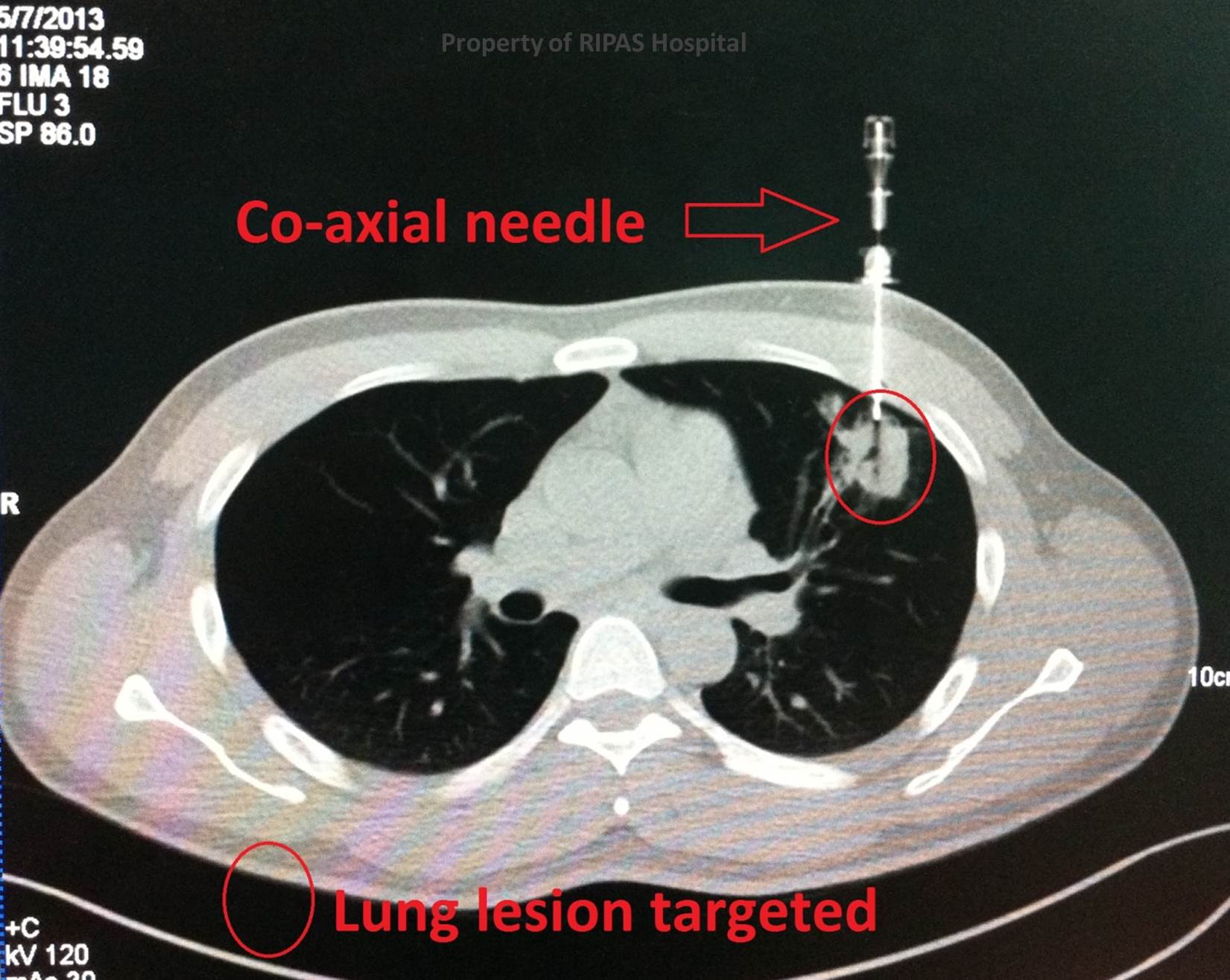
Figure 1b: Annotated CT chest showing fine
needle aspiration of the lung nodule using co-axial needle.
(Click on image to
enlarge) |
|
|
|
Lung lesions are common. Biopsy is frequently required for management purposes.
Biopsy may be performed to determine a histological diagnosis ( i.e TB v
malignancy ) for a lung lesion or to ascertain the specific histology of a lung
cancer to determine treatment.
Lesions may be accessed in 3 ways:
1.
Bronchoscopically
2. Via image
guidance – the vast majority of which require CT guidance
3. Surgical
biopsy/excision
Each patient should be assessed on a case by case basis, ideally with a MDT
meeting discussion.
Bronchoscopic Biopsies
In the presence of either a central lung mass or peripheral lesions (nodules),
bronchoscopy is generally performed to evaluate the status of the endobronchial
epithelium for lesions and resectability. If endobronchial lesions are seen,
then a direct bronchoscopic biopsies of the lesion may be performed under direct
vision. If the lesion is peripheral, then a biopsy forceps can be inserted into
the segmental bronchii where the nodule or mass is located, determined using CT
scan of the lungs, and a blind transbronchial biopsies is performed, although
the yield for this sort of procedure is very low with sensitivity as low as 30%
and specificity as high as 100%. In combination, bronchial brushings and lavage
can also be performed at the culprit bronchus to increase yield of cellular
materials.
In the presence of peri or pre-tracheal or subcarinal enlarged mediastinal lymph
nodes, a transtracheal or transbronchial biopsies of this lymph nodes is
possible using endobronchial ultrasound (EBUS) guidance to locate the lymph
nodes. EBUS-TBNA (EndoBronchial UltraSound – TransBronchial Node Aspiration)
has been shown to have a sensitivity and specificity of 92% and 100%
respectively.
CT guided Fine Needle Aspiration Cytology (FNAC)
There are a number of relative contraindications to CT guided biopsy, which
include:
-
Poor respiratory function. Pulmonary function testing should be performed.
-
An uncooperative patient – if the patient cannot lie still or follow
breathing instructions the procedure is a non-starter. Depending on the
location the patient may have to be prone or supine.
-
No viable safe access to the lesion
-
An uncorrectable coagulopathy
Several issues should also be assessed in planning the procedure
1. Size of lesion
( sub 12mm can be challenging to access )
2. Pleural to
lesion distance. The longer route the more risky
3. Whether a
fissure must be crossed in path to lesion. Pneumothorax more likely.
The main risk factors are pneumothorax and haemoptysis. The former is much
commoner, a percentage of which will be large enough to require a pleural drain.
CT lung biopsy is normally performed with a co-axial needle (typically 18G).
Skin surface markers are sited (Figure x) and a small range of images taken to
determine the access point. Local anaesthetic is applied and a small skin
incision (4-5mm) made.
With the patient breathing normally (no breath hold) the access needle is
angulated and advanced to just prior to the lesion edge (Figures 1 and 2). The
biopsy needle is then passed through the access needle to acquire one or more
samples. Biopsy needle throw is typically 20mm.
After the biopsy is complete a check image is taken to assess for a pneumothorax.
A chest x-ray should then be taken 4 hours after the procedure to check for a
pneumothorax.
Video Assisted Thoracoscopic Biopsies
When the above techniques, bronchoscopic transbronchial or EBUS-TBNA and CT
guided biopsies, failed to confirm a positive diagnosis, then patients are
generally referred to the thoracic surgeon for VATS biopsies of the lung
lesions.
VATS biopsies can be performed through 2 or 3 ports and is generally helpful in
periperal lesion larger than 1cm. Subcentimetre lesions may be difficult to
detect on VATS unless they are near the surface. Likewise, central lesions are
impossible to detect if they are small.
A wedge segment containing the nodule or lung lesion is removed using
endostapler to excise the lung wedge. VATS lung biopsy has a reported
sensitivity, specificity and diagnostic accuracy of 95%, 100% and 97%
respectively.
Images and text contributed and prepared by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
Dr Chong Chee Fui, Thoracic Unit, Department of Surgery,
RIPAS Hospital
All
images are copyrighted and property of RIPAS Hospital.
