IMAGE OF THE WEEK 2013
WEEK 11
TETRALOGY OF FALLOT
|
 |
 |
|
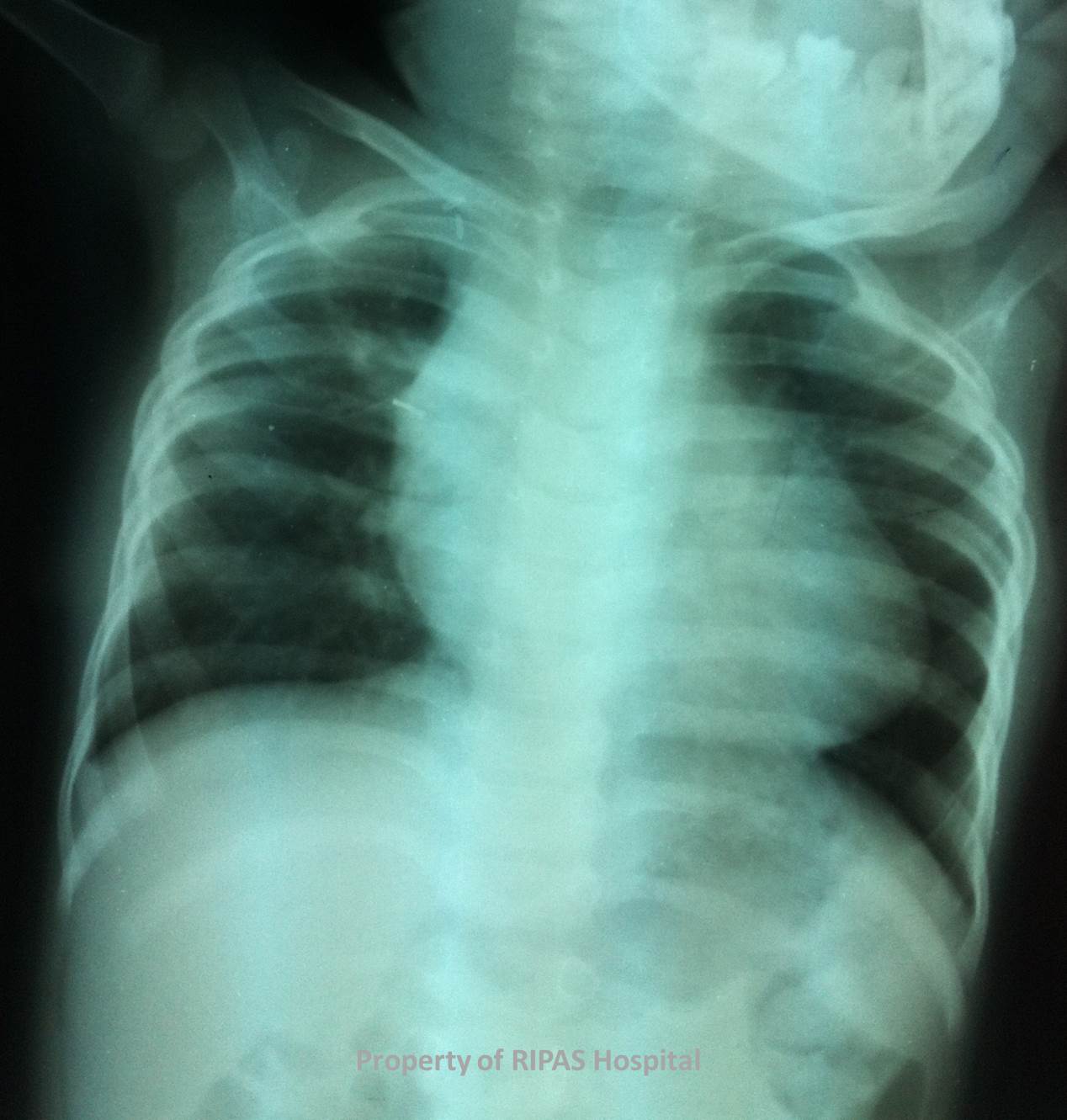
Figure 1a: Chest radiograph showing the classic boot
shaped heart associated with tetralogy of Fallot.
(Click on image to
enlarge) |
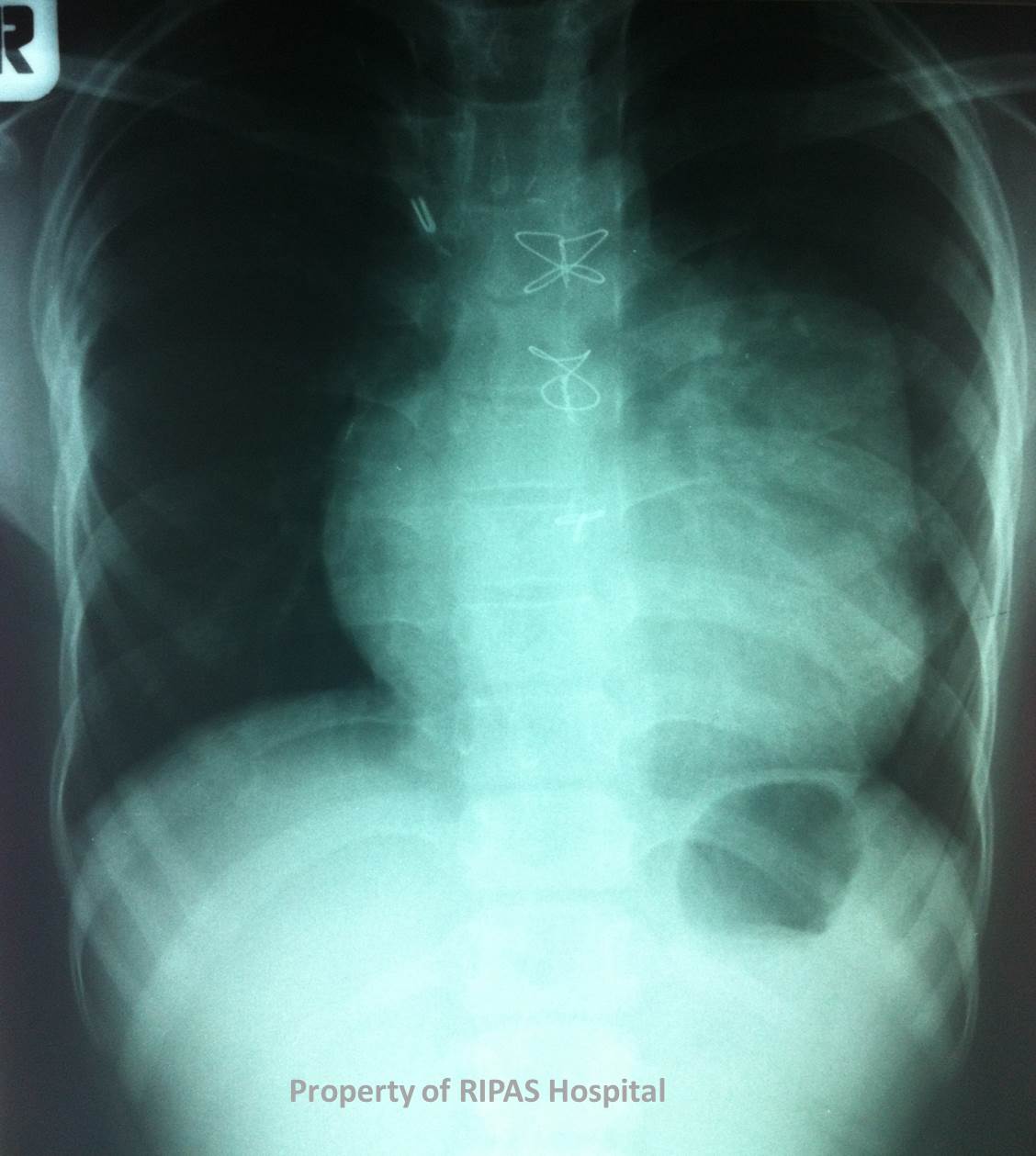
Figure 1b: Chest radiograph of the same infant
after single stage surgical repair as indicated by the sternal wires.
(Click on image to
enlarge) |
|
|
|
Tetralogy of Fallot or Known as TOF in short, is one of the most
common congenital heart disorders, affecting newborn infant.
It is characterized by a tetrad of congenital heart defects which
are right ventricular outflow tract obstruction (infundibular stenosis),
ventricular septal defect (VSD), overriding aorta and RV hypertrophy. The
genesis of these congenital cardiac abnormalities is the results of an anterior
and leftward displacement of the infundibular, or conal septum.
Other associated cardiac abnormalities are atrial septal defect,
patent ductus arteriosus, complete atrioventricular septal defects, multiple
VSDs and less commonly with persistent left SVC, anomalous origin of left
anterior coronary artery and aberrant origin of the right or left pulmonary
artery.
The clinical features of TOF are directly related to the severity
of the anatomic defects and infants often show the following signs and symptoms:
·
Cyanosis, particularly on feeding and crying
·
Difficulty in feeding
·
Failure to thrive
·
Exertional dyspnea, worsening with age, relieved by squatting
·
Most infants are smaller than expected for age
·
Fingers and toe clubbing at 3-6 months of age
·
A systolic thrill along the left sternal border
·
A harsh systolic ejection murmur over the pulmonic area and the left sternal
border
·
RV predominance on palpation
·
A bulging left hemithorax
·
Aortic ejection click
Laboratory investigations usually showed elevated Haemoglobin and
haematocrit in proportion to the degree of cyanosis. Other haematological
abnormalities include decreased clotting factors, low platelet count and
prolonged APTT and INR. SaO2 varies and PCO2 and pH are usually normal.
Imaging studies should include:
·
2D transthoracic echocardiography
o
Usually diagnostic and gold standard for delineating the tetrad of cardiac
deformities as well as other deformities.
·
Chest radiograph
o
Classic boot shaped heart (Coeur en sabot) which is the hallmark of the disorder
(see figure 1)
o
Diminished pulmonary vascularity and diminished prominence of the pulmonary
arteries and trunk.
·
MRI
o
Good modality for delineating the aorta, RVOT, VSDs, RV hypertrophy and the
pulmonary arteries and branches.
o
Getting measurements of intracardiac pressures, gradients and blood flow.
·
Coronary angiogram
o
Ruling out coronary artery anomalies
o
Assessment of pulmonary annulus, and pulmonary arteries, severity of RVOT and
size and location of VSDs.
Current management of TOF is early surgical correction with good
long-term outcomes. Surgical correction is usually performed as single stage
repair at 3-6 months of age. Approach is via a right atriotomy (incision of the
right atrium) which will provide a good view of the VSD, which patched with
pericardium or Teflon patch, correcting the VSD and the overriding aorta. Muscle
bundles at the infundibulum are resected to alleviate the infundibulum
obstruction and lastly for pulmonary stenosis, the pulmonary artery is opened
right down through the pulmonary annulus and a transannular patch is used to
enlarge the pulmonary trunk.
Images contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
Text prepared by
Dr Chong Chee Fui, Thoracic Unit, Department of Surgery,
RIPAS Hospital
All
images are copyrighted and property of RIPAS Hospital.
