IMAGE OF THE WEEK 2013
WEEK 12
AETIOLOGIES OF
INFERIOR VENA CAVA THROMBOSIS (IVCT)
|
 |
 |
 |
|
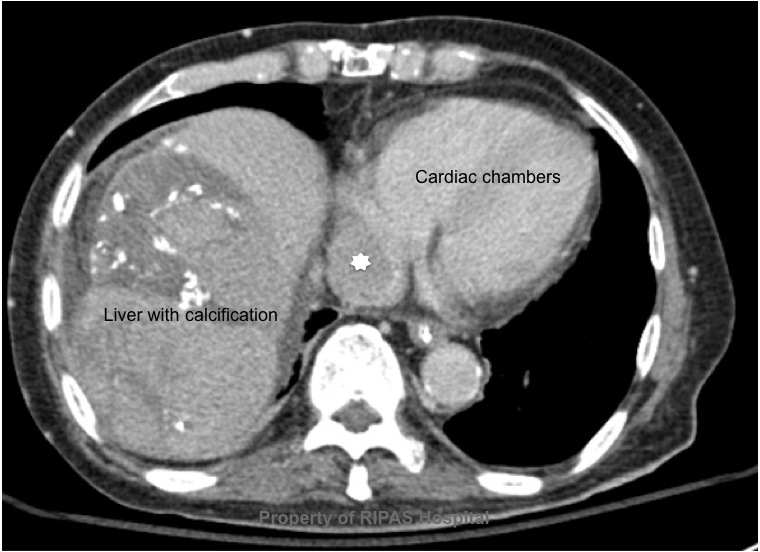
Figure 1a: Transverse sectional cut through the
abdomen at the level of T10, showing a clot in the IVC (white star) just
at the point of entry into the right atrium.
(Click on image to
enlarge) |
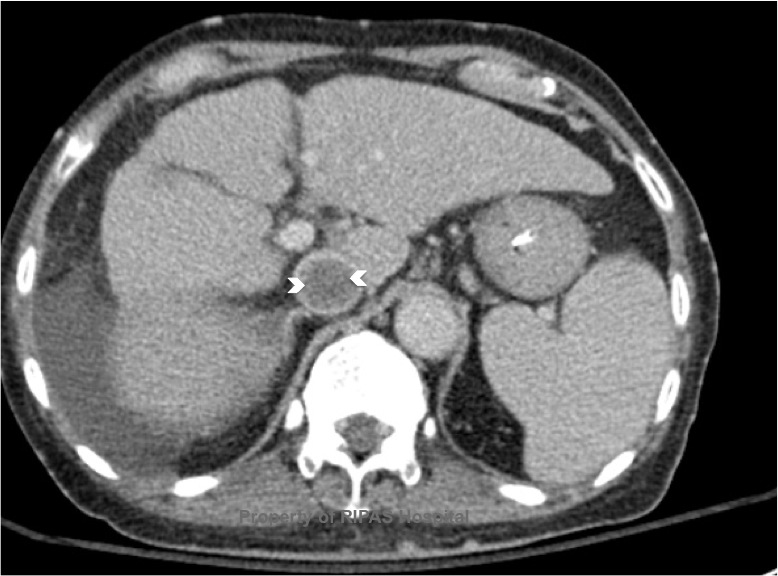
Figure 1b: Transverse sectional cut through the
abdomen at the level of T12, showing a clot in the IVC (white star) with
the 'Polo Mint sign'.
(Click on image to
enlarge) |
Figure 1c: Computer generated coronal section
through level of IVC showing an extensive clot in the IVC (white arrow)
arising just above the origin of the left renal vein.
(Click on image to
enlarge) |
|
|
|
|
The incidence of IVCT is
largely uncertain because of the clinical variability in presentation and its
association with other primary pathologies. However, studies in the USA, have
shown that the incidence of IVCT is estimated at 4-15% in those diagnosed with
Deep Venous Thrombosis (DVT).
The aetiologies of IVCT
are fairly similar to that of DVT in that the factors leading to activation of
the coagulation cascades are contributed by the Virchow’s triad of
hypercoagulability, Haemodynamic (stasis, turbulence) and endothelial
injury/dysfunction. However specific situations relate to IVCT only:
INTRAVASCULAR
AETIOLOGY
•
Tumours - Numerous malignancies have been associated
with IVCT but the most common is the Renal Cell Carcinoma which can invade into
the renal vein, and extend into the IVC causing stasis and obstruction and hence
thrombosis. Other reported malignancies include seminomas, teratomas,
retroperitoneal leiomyosarcoma, adrenal cortical carcinoma, renal angiomyolipoma
and hepatic hemangiomas, either through direct invasion of IVC or external
compression. Most malignancies are a risk factor for DVT through Virchow’s triad
and hence is also a risk factor for IVCT.
•
Dysfunctional coagulation system - Nephrotic syndrome
has been reported to cause IVCT. Other causes to be considered includes
antiphospholipids syndrome, Protein S and Protein C deficiences.
•
Iatrogenic - Recent medical intervention particularly
endovascular involving the IVC has led to an increased recognition of IVCT, such
as long line dialysis catheter, prolonged femoral venous catheters, porta-catheters,
intravenous pacing wires, IVC filters and hepatic transplantation.
•
Medication - oral contraceptives pills.
EXTERNAL AETIOLOGY (via extrinsic compression)
•
Tumours - Most tumours described above can cause
extrinsic ompression of the IVC, leading to IVCT.
•
Extrinsic compression by expanding nearby structures
such as AAA, iliac aneurysms, hepatic abscesses (ameoba or echinococci),
polycystic kidneys, pancreatic pseudocysts and acute pancreatitis have been
reported to cause IVCT.
•
Heamatoma/Trauma - Enlarging retroperitoneal, psoas
or hepatic hematoma adjacent to the IVC as well as direct trauma to IVC
(endothelial injury - one of Virchow’s triad)
•
Pregnancy - the enlarging pregnant uterus can
potentially compressed on the IVC causing extrinsic obstruction and hence IVCT.
•
Congenital absence of IVC - Incidence of anomalies of
IVC is reported at 0.6 - 2% in the presence of other cardiovascular defects.
Individuals tend to present with DVT at a young age.
IMAGING
As shown in Figure 1a, 1b
and 1c (CT scan), the thrombus occupies almost 90% of the lumen with a
peripheral ring of blood flow as indicated by the contrast (Figure 1b), a sign
know as the ‘Polo Mint Sign’. In this patient, the thrombus continue upwards
into the right atrium (Figure 1c) and is at risk of embolisation into the
pulmonary vasculature causing PE.
Images contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
Text prepared by
Dr Chong Chee Fui, Thoracic Unit, Department of Surgery,
RIPAS Hospital
All
images are copyrighted and property of RIPAS Hospital.
