
Figure 1: The most sensitive imaging investigation to detect calculi
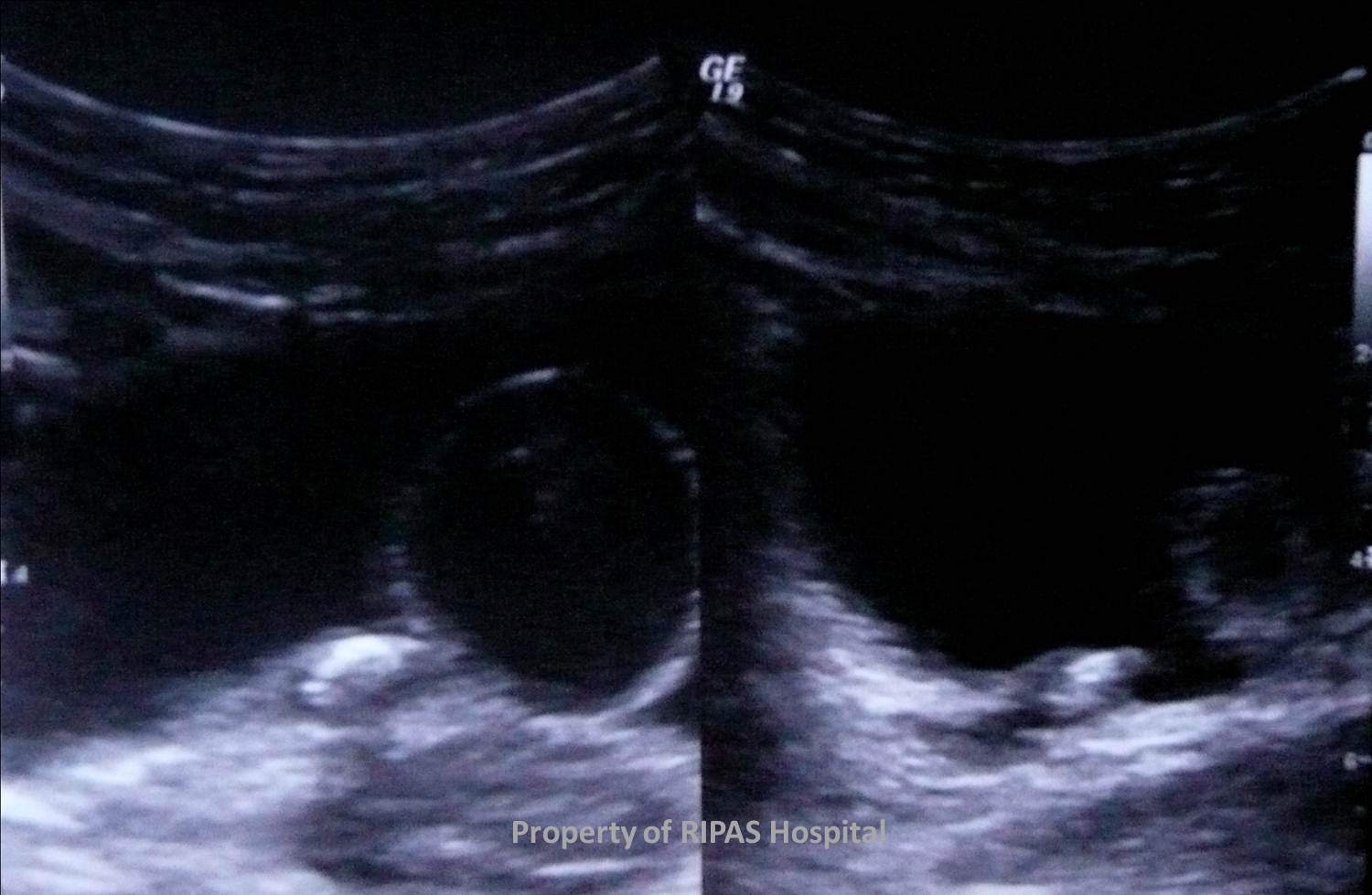
Figure 2: It can identify ureteric calculi (ultrasound almost never can unless at the extreme VUJ).






If not – repeat CT-KUB should be performed.
IMAGE OF THE WEEK 2012
WEEK 14
BRUNEI - HOME OF RENAL CALCULI
Big ones. Small ones. Solitary ones. Multiple ones…. Brunei is the home of renal calculi.
How can imaging help and how can it be used. What pathology can be seen?
The overwhelming answer is CT-KUB. This non contrast study allows for the detection of 99% of all calculi, even as small as 1mm. It has multiple advantages, such as:
|
|
Figure 1: The most sensitive imaging investigation to detect calculi |
|
|
|
Figure 2: It can identify ureteric calculi (ultrasound almost never can unless at the extreme VUJ). |
|
|
|
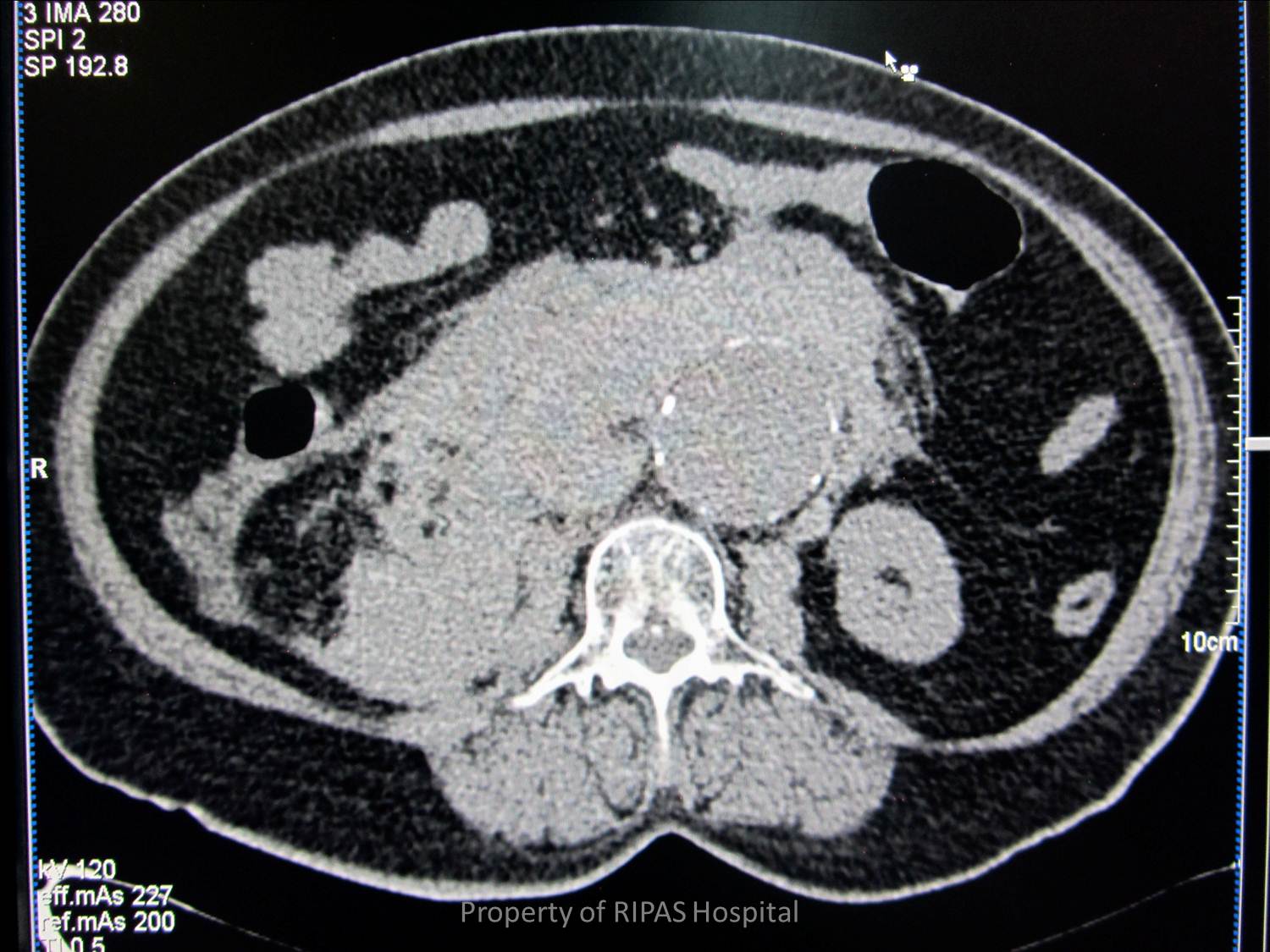
Figure 3: Complications can be seen, such as hydronephrosis, perirenal abscesses, a urinoma or xanthogranulomatous pyelonephritis. | |
|
|
Figure 4: Alternative causes for presume renal colic can be found, such as an abdominal aortic aneurysm rupture or pancreatitis. | |
|
|
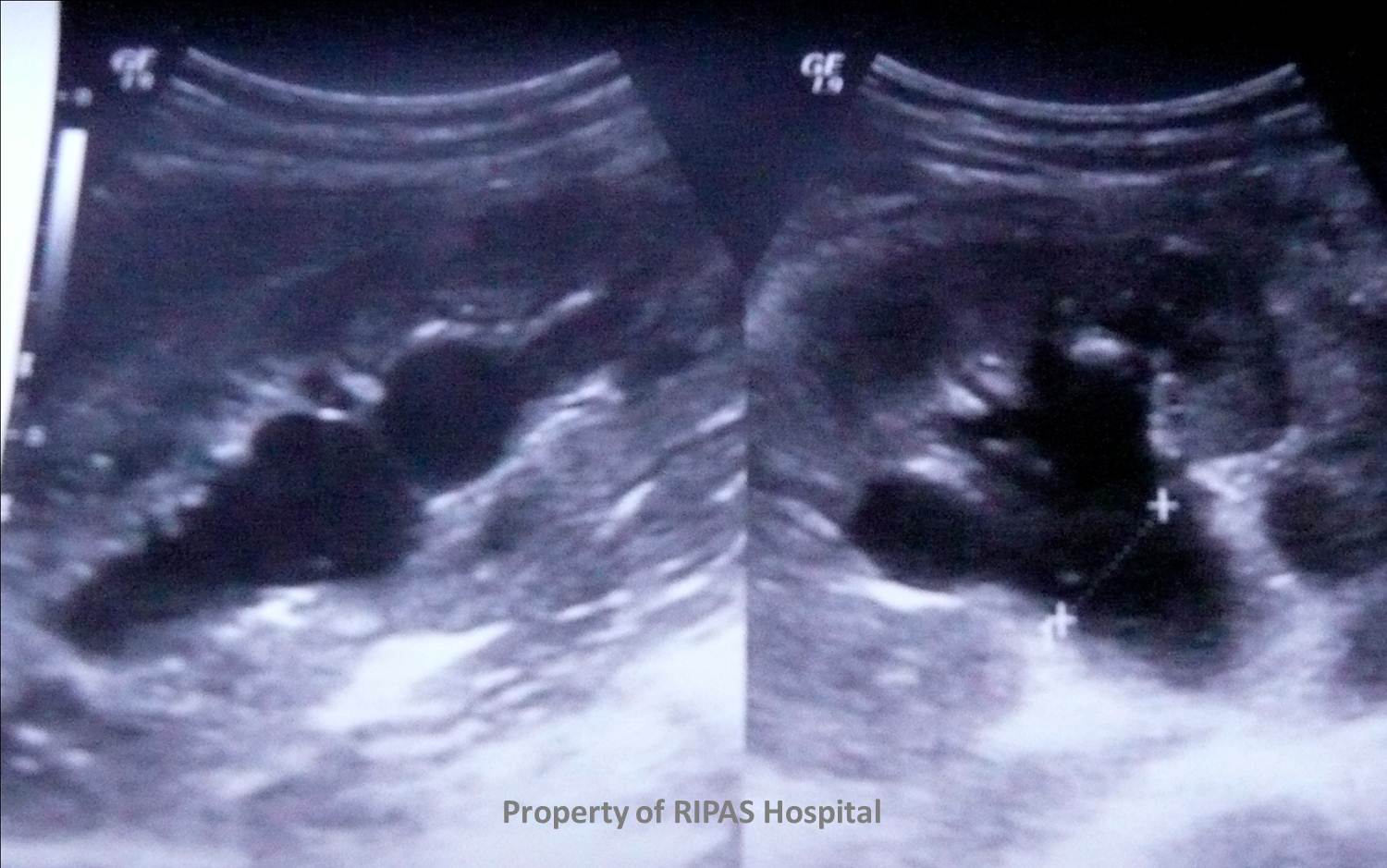
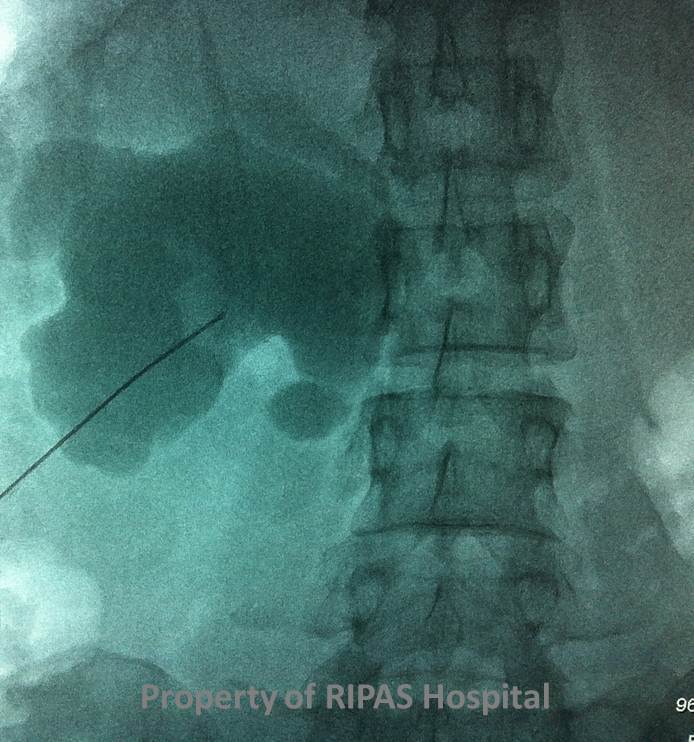
Figure 5: Ultrasound’s role is more to assess for hydronephrosis, especially if a nephrostomy is to be undertaken, as the renal puncture is normally performed under ultrasound guidance. | |
|
|
Figure 6: Ultrasound’s role is more to assess for hydronephrosis, especially if a nephrostomy is to be undertaken, as the renal puncture is normally performed under ultrasound guidance. | |
|
|
Figure 7: It may identify stones, especially larger ones, but is not the preferable imaging modality. It also has a role when the patient has haematuria as the cause maybe a renal tumour, bladder tumour or other rather than a calculus. | |
|
|
Figure 8: But don’t forget the humble plain film (KUB). This should always be done first, identifying more than 50% of renal calculi, largely due to the commonest calculi being composed of calcium and hence radio-opaque. | |
|
|
Figure 9: But don’t forget the humble plain film (KUB). This should always be done first, identifying more than 50% of renal calculi, largely due to the commonest calculi being composed of calcium and hence radio-opaque. | |
|
|
Figure 10: Bladder calculi may also be observed. | |
|
|
Figure 11:
If the stone was visible on KUB – then a further KUB is suitable for
follow up. If the stone was detected on the CT-KUB the scanogram/scout
(essentially like a normal KUB) of the study should be reviewed – if it
was visible on this the stone can be followed up with a KUB film.
If not – repeat CT-KUB should be performed. |
Image and text contributed and prepared by
Dr Ian Bickle, Department of Radiology, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()