IMAGE OF THE WEEK
WEEK 17
|
|
|
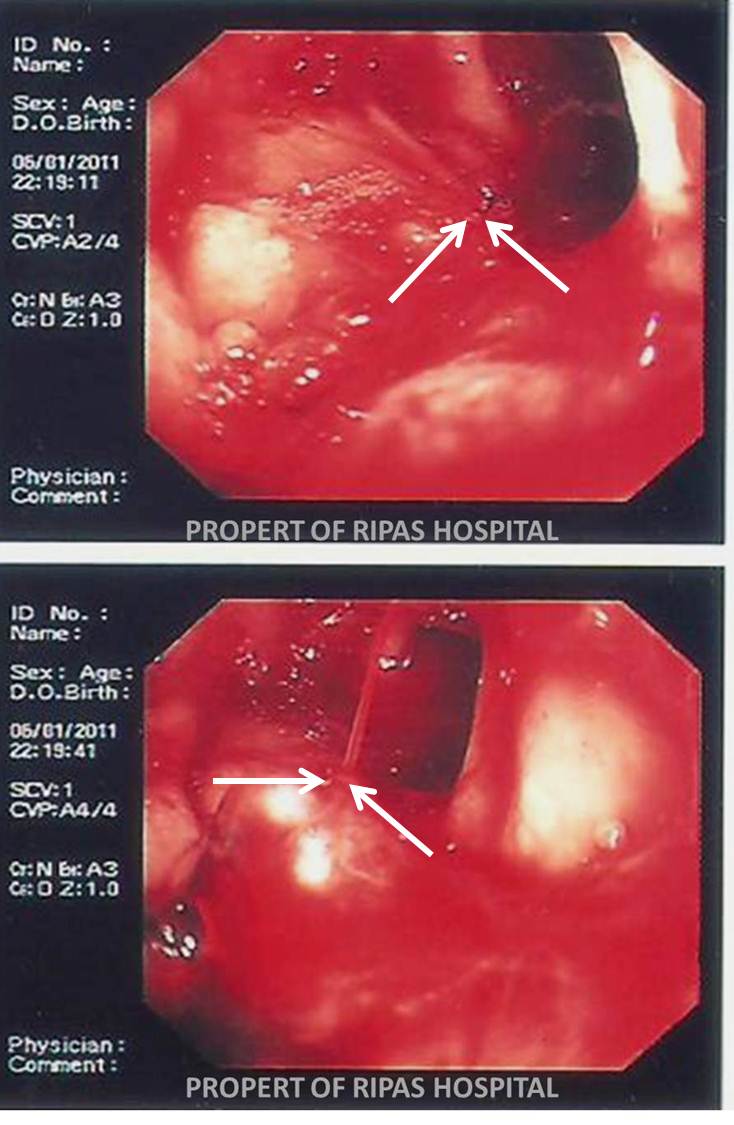
BLEEDING DUODENAL ULCER
This patient had a bleeding duodenal ulcer that is categorised as Forrest Ia lesion (a spurting artery as indicated by the white arrows).
The Forrest Classification which describes the endoscopic lesions visualised during endoscopy are widely used for predicting the risk of rebleeding if no endoscopic treatment is provided.
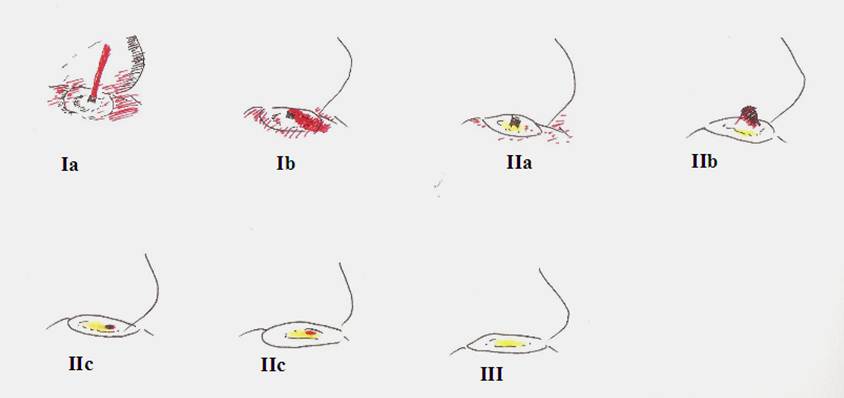
FORREST CLASSIFICATION
|
Types of lesion |
Description |
Rebleeding rate |
|
Type I: Active bleeding |
||
|
Ia |
Spurting artery |
55-100% |
|
Ib |
Oozing |
|
|
Type II: Recent bleed |
||
|
IIa |
Non bleeding vessel |
40-50% |
|
IIb |
Adherent clot |
20-30% |
|
IIc |
Haemetinic spots (red or black spot) |
10% |
|
Type III: Lesions without bleeding |
||
|
III |
Clean base |
<5% |
Apart from predicting rebleeding rate, the Forrest Classification also predicts the mortality rate; 11% for active bleeding (Forrest Ia and Ib), 11% for visible vessel (Type IIa), 7 percent for adherent clot, 3 percent for haemetinic spot (Type IIc) and 2 percent for clean base (Type III).
Other criteria used for predicating risk of upper gastrointestinal bleeding and mortality are the Rockall score (utilises clinical and endoscopic criteria) and Glasgow Blatchford (utilises clinical and laboratory parameters) score. The Rockall Score is particular useful for predicting mortality whereas the Glasgow Blatchford score is good for predicting early discharge or requiring for hospital admission.
Forrest Classifications lesions types Ia, Ib, IIa and IIb are considered high risk for rebleeding and require endoscopic treatment. Recommended treatments require two prong approach; adrenaline or sclerosant injections with coaptive coagulation or haemoclip. Monotherapy in particular with adrenaline or sclerosant injections is associated with high risk of rebleeding.
Failing endoscopic therapy twice is considered an indication for alternative therapy: angiography with embolisation or surgery.
In addition to the endoscopic therapy, all patients with upper gastrointestinal bleeding not suspected to be variaceal in origin should receive intravenous proton pump inhibitor (i.e. intravenous omeprazole 80 mg bolus followed by 8 mg/hr infusion for up to three days). The infusion can be stopped sooner if patient is stable without evidence of rebleeding. This should be later converted to oral proton pump inhibitor and this can be sooner. It is important to check for helicobacter pylori infection.
Diagrammatic representation of the various type of Forrest lesions
|
|
Images prepared by Dr Vui Heng Chong, Consultant Gastroenterologist and Hepatologist, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()