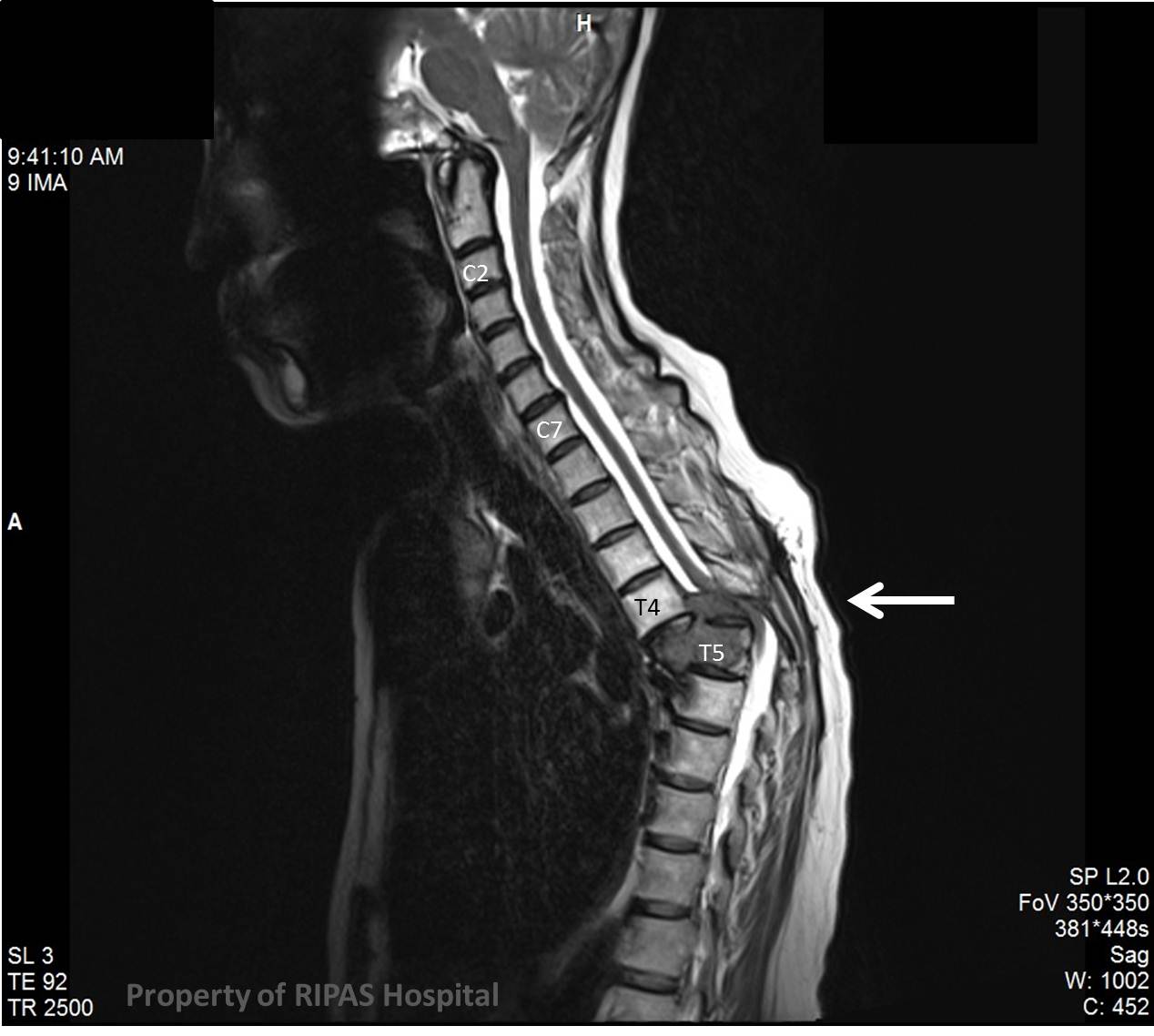
Figure 1: MRI of the spine (saggital section) showing pathological fracture dislocation of Thoracic vertebra T5 posteriorly and compressing on the spinal cord (Click on picture to enlarge)
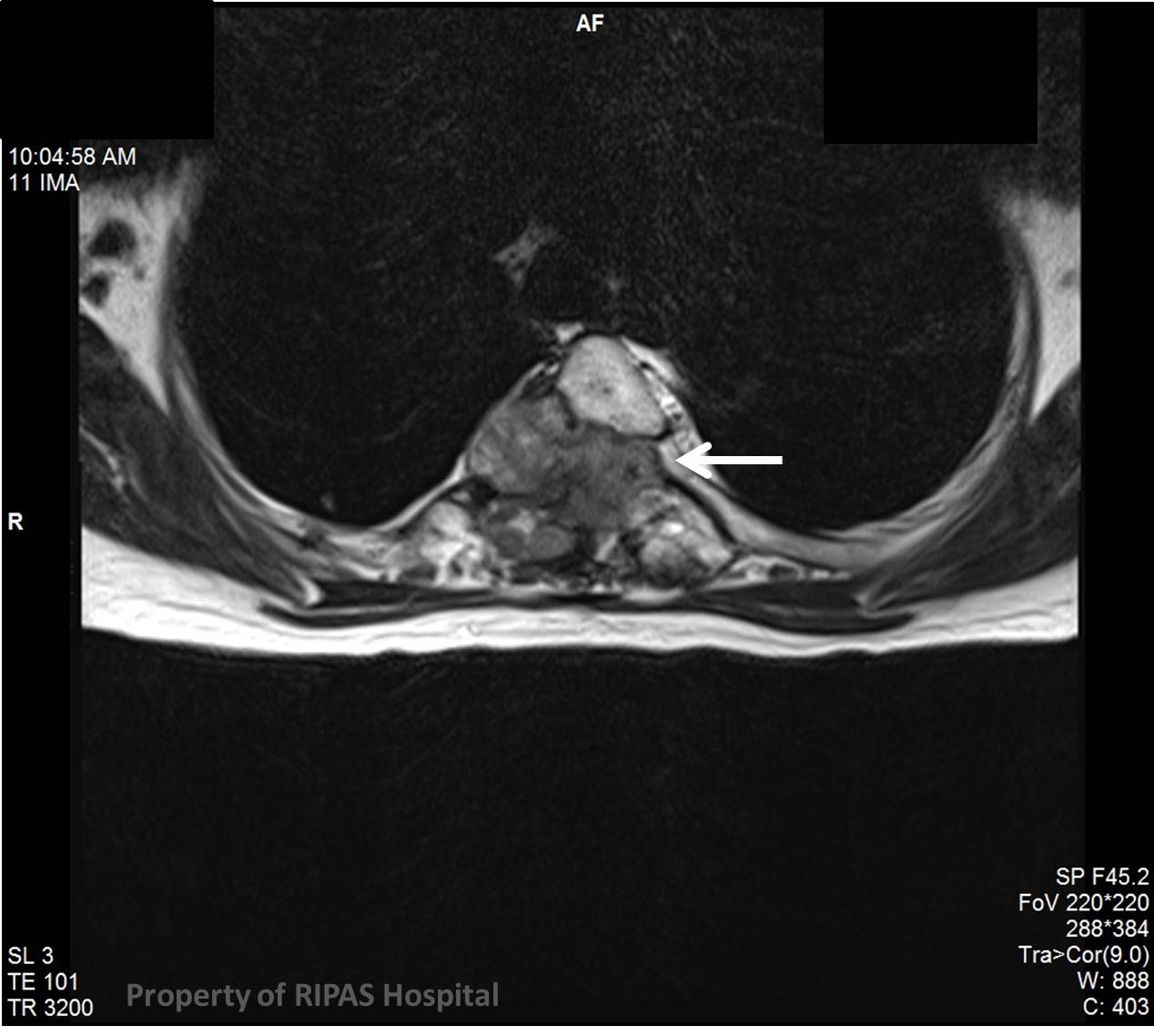
IMAGE OF THE WEEK 2012
WEEK 17
SPINAL CORD COMPRESSION
|
|
Figure 1: MRI of the spine (saggital section) showing pathological fracture dislocation of Thoracic vertebra T5 posteriorly and compressing on the spinal cord (Click on picture to enlarge) |
|
|
|
Figure 2: MRI of the spine (transverse section) showing tumour (thyroid carcinoma metastasis - white arrow) invading and destroying the T5 vertebral body with compression of the spinal cord (Click on picture to enlarge) |
Spinal cord compression is a medical emergency and occurs as a
result of compression of the spinal cord (Figure 1 white arrow
) by bone fragments from a vertebral fracture, ruptured vertebral disc, an
abscess, a tumour or metastases (Figures 1 and 2). Symptoms suggestive of spinal
cord compression include an acute onset of back pain, dermatone of increased
sensation, paralysis below the level of compression, urinary and fecal
incontinence or retention. Lhermitte’s sign (intermittent shooting pain) and
hyperreflexia may be present.
Urgent radiological investigations are required usually with MRI
as shown above of the whole spine (Figure 1
). The most common causes of cord compression are tumours such as lung cancer
(non-small cell lung cancer), breast cancer, prostate cancer, renal cell
carcinoma, thyroid carcinoma, lymphoma and multiple myeloma. Infective causes
include abscesses and granulomas such as tuberculosis. The case above was due to
a thyroid carcinoma bony metastasis to vertebral body T5 resulting in
destruction of the body of the vertebra and subsequent posterior dislocation of
T5, resulting in compression of the spinal cord.
Once diagnosis is confirmed, dexamethasone is given intravenously
to reduce the peri-lesion oedema and hence relieved the compressive pressure off
the cord.
Emergency radiotherapy (20Gy/5fractions, 30Gy/10fractions, or 8Gy/1fraction) is
the mainstay of treatment for malignant spinal cord compression in centres where
radiotherapy is available. If this is not available, then decompressive surgery
is the main stay of therapy in order to prevent permanent neurological damage to
the cord and permanent paralysis. Surgery is also indicated if permanent
paralysis has occurred for pain controlled. Post-operative radiation is
delivered within 2-3 weeks of surgical decompression as adjuvant therapy for the
tumour.
The median survival of patients with metastatic spinal cord compression is about 12 weeks, due to the advanced nature of the underlying malignant disease.
Image contributed and prepared by
Dr Ian Bickle, Department of Radiology,
Text prepared by
Mr William Chong, Department of Surgery,
RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()