IMAGE OF THE WEEK
WEEK 18
|
|
|
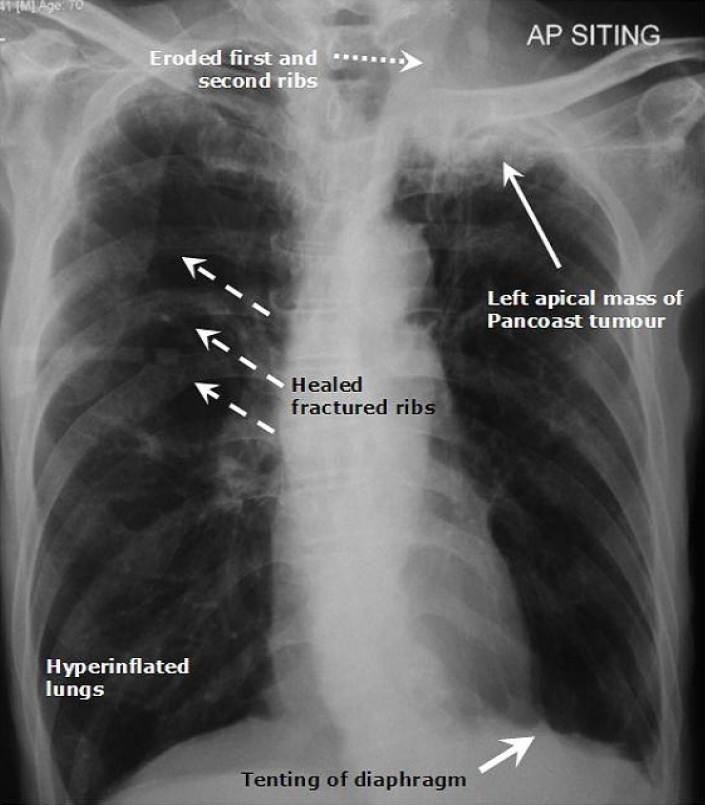
PANCOAST TUMOUR
The chest radiography shows a tumour in the apex of the left lung (left Pancoast tumour) with ribs destructions and healed fractured ribs on the right side in the setting of hyper-inflated lungs with tenting of the diaphragm consistent with emphysematous type of chronic obstructive pulmonary airway disease (COPD).
Pancoast tumour (pulmonary sulcus tumour or superior sulcus tumour) refers to any pulmonary tumour that is located at the apex of the lung. Pancoast tumour accounts for 1-3% of all lung cancers. It is usually non-small cell carcinoma (mostly squamous cell or adenocarcinoma with oat cell accounting for 3-5%). The tumour is named after a prominent US radiologist, Henry Pancoast who first described them in 1924 and 1932.
It is more common in male and in those who smoke. Generally, the risk factors are similar to that of other lung cancer.
The tumour may invade soft tissue structures such as vascular (brachiocephalic and subclavien arteries) and nerves (nerve roots, lower plexuses of the brachial plexuses, phrenic nerve, and sympathetic chains) and bony structures such as ribs or vertebra. Invasion of the phrenic or recurrent laryngeal nerves or involvement of the superior vena cava is not representative of classic case of pancoast tumour. Invasion of the sympathetic chains or ganglion lead to the well known Horner’s syndrome: enophthalmos (sunken eye), anhidrosis (lack of or reduced sweating), meiosis (constricted pupils) and ipsilateral partial ptosis (droopy eyelid).
Clinical symptoms include dyspnoea secondary to the underlying lung disease (COPD) or tumour and pain in association with local tissue spread- bone pain (shoulder pain or scapula) or neuralgic pain (pain along nerve distribution i.e. ulnar nerve) characteristically in the distribution of eighth cervical or first or second thoracic trunk distributions. Clinicians need to be aware of the less common paraneoplastic manifestations, mainly metabolic that include Cushing syndrome, excessive antidiuretic hormone secretion, hypercalcemia, myopathies, haematological problems, and hypertrophic pulmonary osteoarthropathy (HPOA).
Images prepared by Dr Vui Heng Chong, Consultant Gastroenterologist and Hepatologist, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()