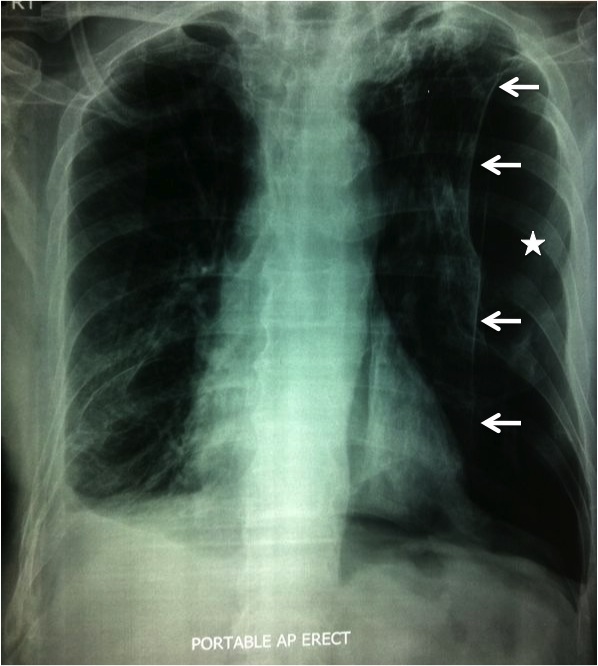
Figure 1: Trapped lung
(lung margins indicated by white arrows) with persistent pneumothorax
(white star).
(Click on image to enlarge)
IMAGE OF THE WEEK 2013
WEEK 2
Trapped lung or lung entrapment
|
|
|
|
Figure 1: Trapped lung (Click on image to enlarge) |
Trapped lung or unexpanded lung is defined as the failure of the lung to fully expand to the chestwall, resulting in a persistent pneumothorax or space in the pleural space. The mechanism of the trapped lung is usually either due to visceral pleural restriction or from endobronchial obstruction resulting in lobar collapse. The differentiation of trapped lung from lung entrapment is the presence of active pleural inflammation or pleural malignancies in the latter. Lung entrapment occurs during the acute phase of the active pleural inflammation but once the inflammation resolves usually after antibiotic therapy, the visceral pleural undergoes thickening from fibrous organisation resulting in trapped lung.
In Brunei, the most common cause of a lung entrapment is empyemas following incompletedly treated parapneumonic effusion. Other causes of lung entrapment include coronary artery bypass graft surgery, postcardiac injury syndrome, complicated parapneumonic effusions, uremia, radiation therapy and rheumatoid pleurisy.
Trapped lung is the end stage of fibrinous or granulomatosis pleuritis in which a mature fibroelastic layer develops along the visceral pleural surface, thus impeding normal lung expansion. Usually there is a small to moderate amount of a stable pleural effusion, which is usually sterile.
|
Differences between Trapped Lung with Lung Entrapment as proposed by Moore and Thomas. |
||
|
|
Trapped Lung |
Lung Entrapment |
|
Pathogenesis |
Remote pleural inflammation or blood |
Active pleural inflammation, blood or malignancy |
|
Causes |
Post-CABG, prior empyema, hemothorax, uremia, radiation, rheumatoid pleuritis |
Post-CABG, prior empyema, hemothorax, uremia, radiation, rheumatoid pleuritis |
|
Pleural Fluid Analysis |
Paucicellular, lymphocyte predominant transudate, protein discordant exudates common |
Polymorphonuclear or lymphocyte pre-dominant, concordant exudate |
|
Initial Mean Pleural Pressure |
Usually negative, can be positive |
Usually positive |
|
Pressure/Volume curve |
Monophasic with PEL>14.5 cm H2O/L |
Biphasic with terminal PEL> 14.5 cm H2O/L |
|
Treatment |
Observation for asymptomatic; decortication for symptomatic after parenchymal fibrosis on chest CT scan rule out |
Treatment of underlying condition associated with lung entrapment; in the setting of malignancy, chronic indwelling catheters are recommended if dyspnoea improves with fluid removal |
Treatment of trapped lung or lung entrapment generally involves surgery in the form of decortication in order to preserve lung volume and function. Chronic lung entrapment or trapped lung can result in interstitial lung changes/fibrosis which may result in lost of some degree of pulmonary function. In most instances, removing the fibrinous visceral peel in lung entrapment can resolve the problem with the lung usually achieving full expansion. In trapped lung however, on occasions, the underlying lung may not fully expanded despite removing the thickened visceral pleural. This is usually due to the presence of intersitial lung fibrosis resulting from chronic restriction by the visceral pleura. In this situation, crushing the phrenic nerve may help to reduce the pleural space by elevating the diaphragm and thus removing the residual space. Alternatively, a more drastic approach would involved thoracoplasty with removal of several ribs in order to reduce the pleural space.
Images and text contributed and prepared by
Mr Chee Fui Chong, Department of Surgery.
All images are copyrighted and property of RIPAS Hospital.
![]()