Figure 1: A long clot extracted from an emergency embolectomy/thrombectomy of an acute ischemic right leg. (Click to enlarge picture)
IMAGE OF THE WEEK 2012
WEEK 20
ACUTE ISCHEMIC LEG
|
|
Figure 1: A long clot extracted from an emergency embolectomy/thrombectomy of an acute ischemic right leg. (Click to enlarge picture) |
Acute ischaemic limb is a serious surgical condition characterized by sudden cessation of perfusion of the affected limb resulting in a potential threat to limb viability.
Usual etiologies of acute arterial occlusion includes:
· embolisation of a thrombus from a distant source usually of cardiac origin,
· embolisation from a peripheral aneurysm with embolus or thrombus,
· acute thrombosis of a previously patent but diseased limb artery with critical stenosis (peripheral vascular disease),
· Trauma (including iatrogenic such as dissection following catheterization),
· Reconstruction/graft thrombosis.
Clinical presentation include a sudden onset of severe leg pain, usually patient’s may have complained of intermittent crampy pain in the calf/ves, with a pale, pulseless, painful, cold, mottled or blue, numb (paraesthesia), immobile limb (paralysis). Clinical evaluation should target towards previous history of intermittent claudication suggestive of peripheral vascular disease, other atherosclerotic disease such as stroke, coronary heart disease with chest pain, hypertension, diabetes, hypercholesteraemia, smoking and family history of cardiovascular disease, strokes, blood clots or amputation.
Investigations should aim towards a diagnosis as well as preparing the patient for emergent embolectomy or thrombectomy, These will include a FBC, Renal panel, clotting screen, ECG, CXR, Doppler ultrasound if time permits but more important an angiogram which should include the distal aorta, bifurcation and all the way down to the pedal vessels of the affected limb. If there is a history of intermittent claudication of the contralateral limb, then angiogram of the contralateral should be included. Alternatively, a CT angiogram is just as good using the 64 slice CT as shown in figures 2a&b. For patient with renal failure, a MRA can be requested. Other investigations should aim to exclude a hypercoagulable state such as anticardiolipin antibodies, Protein C & S deficiencies, and anti-factor V antibodies.
|
|
Figure 2: CT angiogram showing an absence of flow in the right common iliac artery as indicated by the white arrow. The wall of the common iliac artery aslo showed calcification indicating presence of peripheral vascular disease. (Click on picture to enlarge) |
|
|
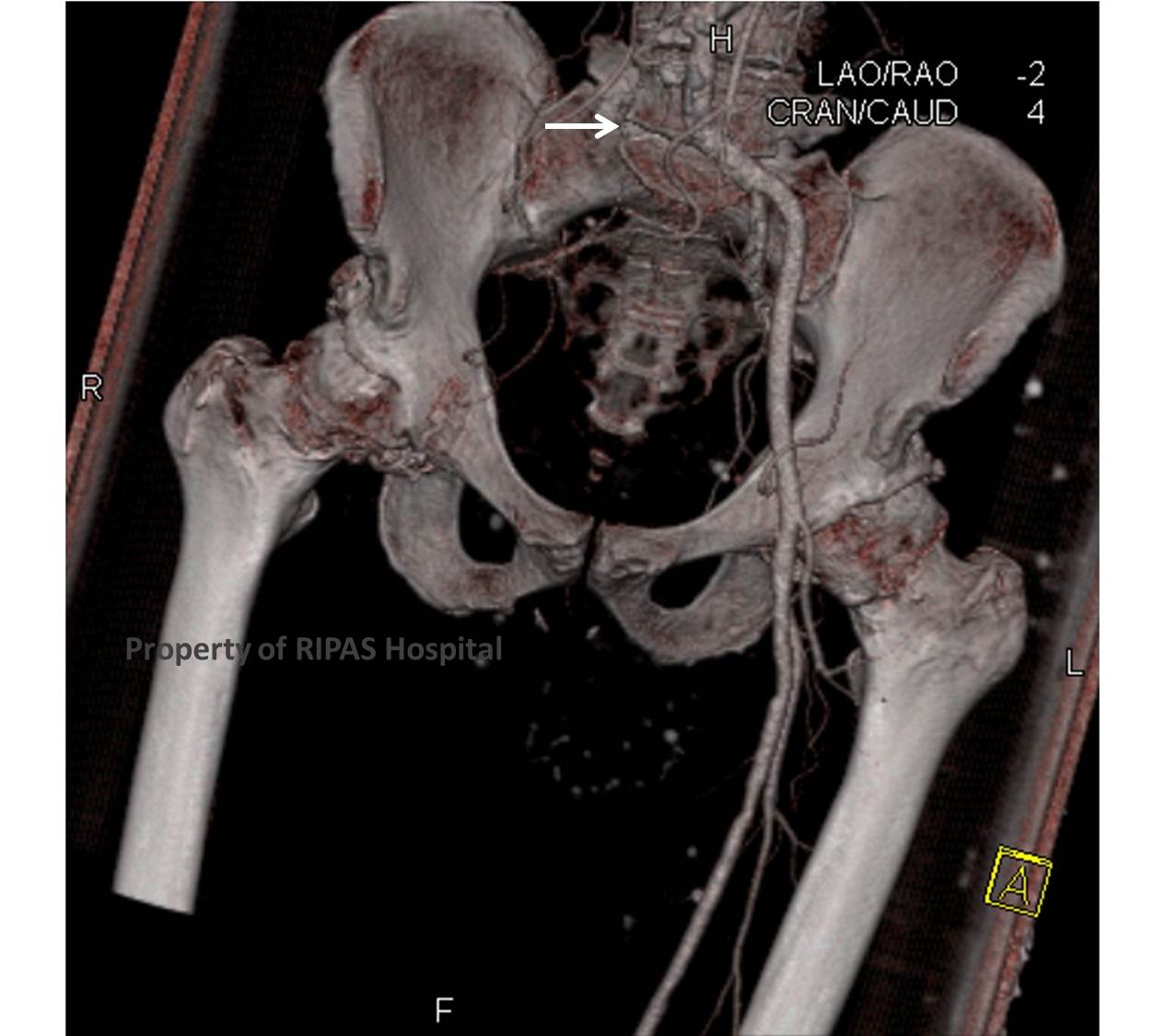
Figure 2b: CT angiogram 3D reconstruction showing an absence of flow in the right common iliac artery (white arrow) and beyond indicating an acute arterial occlusion. (Click on picture to enlarge) |
This condition is a surgical emergency in order to salvage the limb and patient should undergo emergency femoral embolectomy and or thrombectomy. The case above was a native right common iliac artery thrombosis in the presence of a critical stenosis of the origin of the right common iliac artery. A long clot was retrieved during the surgery (figure 1) and the stenosis was noted as an inability to pass the embolectomy catheter up beyond the aortic bifurcation with very poor antegrade flow. A fem-fem crossover graft was performed to bypass blood from the contralateral left common femoral artery to perfuse the right leg. Decision for immediate fasciotomy of the affected calf should be considered if the presentation is more than 12-24 hours old.
Post operatively patient should be started on iv heparin to maintain patency of the graft which should be converted to oral anticoagulation therapy with Warfarin for 3-6 months or indefinitely if any of the investigations for hypercoagulable state was positive.
Images contributed and prepared by
Dr Ian Bickle, Department of Radiology,
and text contributed by Mr William Chong, Department of Surgery
All images are copyrighted and property of RIPAS Hospital.
![]()