
Figure 1a
Figure 1b
IMAGE OF THE WEEK
WEEK 20
|
|
|
|
|
Figure 1a |
Figure 1b |
EUS IMAGING OF GASTRIC CARCINOMA
The endoscopic image shows a type IIa + c gastric lesion, approximately two to three centimeter located over the incisura (Figure 1a&b). Biopsy showed adenocarcinoma that was reported to be well differentiated.
Gastric carcinoma can be classified based on their endoscopic appearances. The Japanese Research Society for Gastric Cancer classification classified gastric cancers into six types (Table 1). The superficial types can have combined features, elevated and ulcerated or depressed centre, as in the present case. Depressed or ulcerated lesions indicated likely submucosa involvement or beyond.
|
Table 1: Japanese Research Society for Gastric cancer classification |
|
| Types | Description |
| Type 0 | Superficial Type |
|
Subtypes - Type 0 I |
Protruding |
|
Subtypes - Type 0 IIa |
Superficial Elevated |
|
Subtypes - Type 0 IIb |
Superficial Flat |
|
Subtypes - Type 0 IIc |
Superficial Depressed |
|
Subypes - Type 0 III |
Exulcerated (excavated and ulceration) |
| Type 1 |
Polypoidal tumours sharply demarcated from the surrounding mucosa, usually attached on a wide base |
| Type 2 |
Ulcerated carcinomas with sharply demarcated and raised margins |
| Type 3 | Ulcerated carcinomas without definite limits, infiltrating into the surrounding walls |
| Type 4 |
Diffusely infiltrating carcinomas in which the ulceration is usually not a marked feature |
| Type 5 | Tumours that cannot be classified into any of the above |
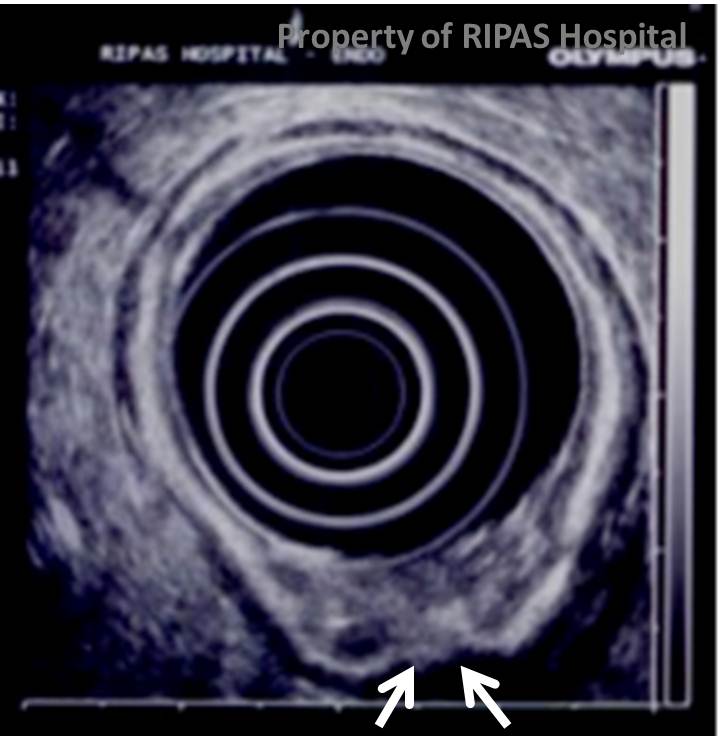
Endoscopic ultrasound shows that the tumour has affected the submucosa (hyper echoic third layer) with breech of some areas (arrows) to affect the muscularis propria layer indicating a T2 lesion. This make it unresected endoscopically with either endoscopic mucosa resection (EMR) or endoscopic submucosa dissection (ESD) due to the risk of perforation. However, it certain specialized centre, this type of lesions is still considered resectable. Lesions located within the mucosa (T1m) or not breeched the submucosa layer (T1sm) can be safely resected endoscopically with either EMR or ESD. On endoscopic ultrasound, the gastric mucosa appears as five layers (Table 2) but can be more, seven if higher frequency imaging is used. EUS is the best modality for local T staging (Table 2).
|
Table 2: T staging of tumour |
|
| Types | Description |
| T1m | Localised to the mucosa |
| T1sm | Localised to the submucosa |
| T2 | Breeched of submucosa but not the serosa |
| T3 | Breeched of serosa |
| T4 | Extension into surrounding structure (i.e. pancreas, liver, vessels etc..). |
Unfortunately, most gastric carcinomas present late and are diagnosed at advanced stages that cannot be treated with curative intent. For case that are still treatable (no evidence of ascitis or metastases), surgical resection with dissections of the peri-gastric lymph nodes (D2 dissection) provide the best chance. The similar situation is true for our local setting in Brunei Darussalam with most the gastric cancers encountered diagnosed either in the advanced stages with metastases or is locally advanced and are categorised as types 2 to 4.
Images prepared by Dr Chong Vui Heng, Consultant Gastroenterologist & Hepatologist, Department of Gastroenterology & Hepatology, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()