
Figure 1a
Figure 1b
IMAGE OF THE WEEK
WEEK 21
|
|
|
|
|
Figure 1a |
Figure 1b |
EUS IMAGING OF COMMON BILE DUCT STONES
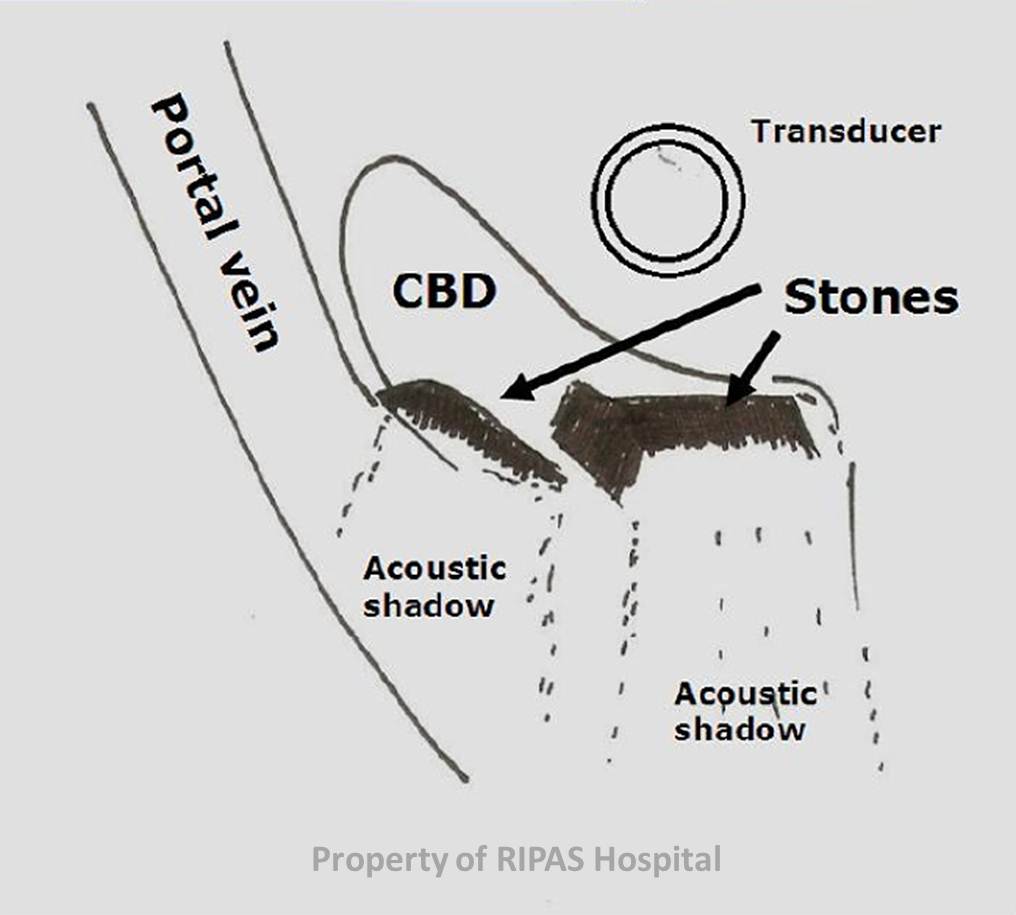
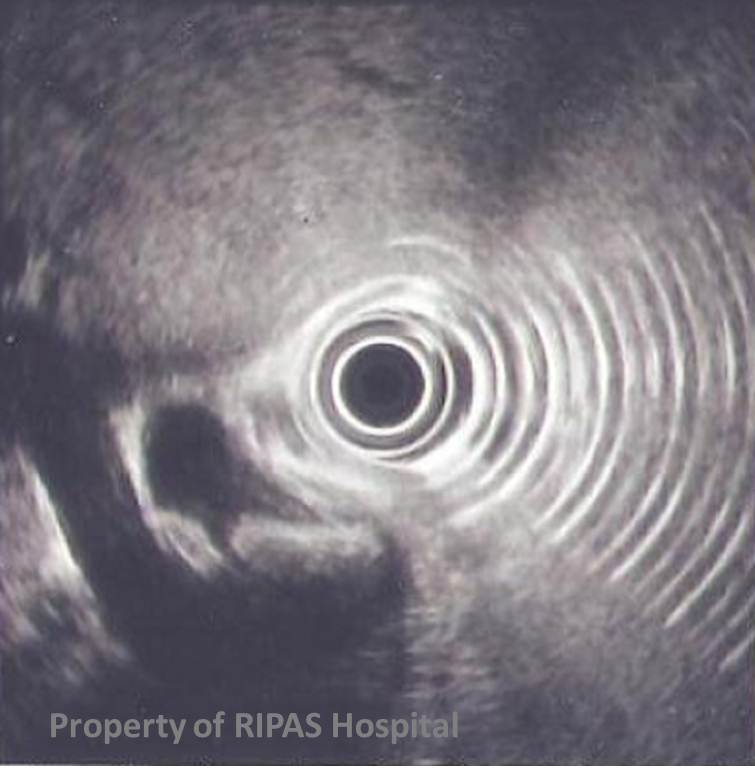
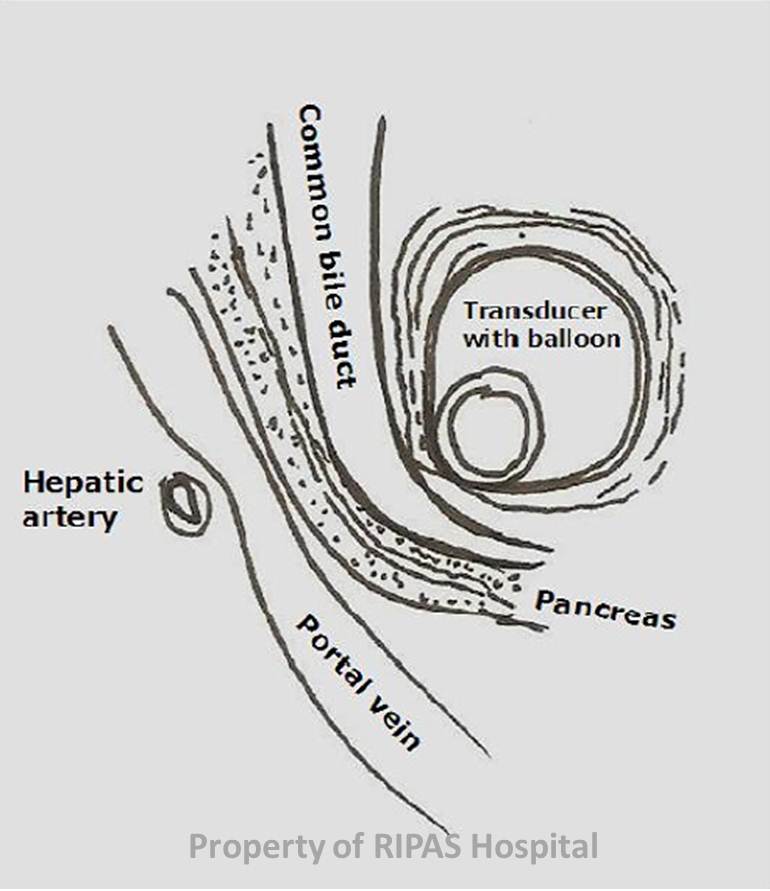
Since its introduction in the early 1980s Endoscopic ultrasound (EUS) has gained popularity with the improvement of imaging, flexible endoscopes and larger channels to allow biopsies and interventions. EUS using 7.5 MegaHz frequency and 9 cm diameters (4.5 cm scan radius) is shown above (Figure 1a&b). EUS scan showed a dilated common bile duct (CBD) a hypoechoic tubular structure nearer to the transducer with hyperechoic structures within the CBD casting acoustic shadows. The portal vein is the tubular structure behind the CBD. A diagrammatic representation is shown below (Figure 2a). Figure 2b show the normal anatomy of the distal common bile duct area.
|
|
 |
|
Figure 2a: Diagrammatic representation of the EUS image showing distal common bile duct viewed from within the duodenum with stones casting acoustic shadows. |
Figure 2b: Distal common bile duct, pancreatic duct and the portal vein all in one view forming the ‘Stack sign’ (view from within the duodenum). |
EUS is particular good for examinations of structures close to the GI lumen and the role of EUS are well defined and evaluation of certain upper GI pathologies (Table 1). The indications for EUS continue to increase as the endoscope technology, accessories and our knowledge improve.
Use of EUS in the management of choledocholithiasis is particularly good for the low or moderate probability for CBD stones (i.e. normal US scan but abnormal cholestatic liver profile). Those with high probability (abnormal US scan and abnormal liver profiles should just proceed directly to ERCP). EUS can obviate the need for any ERCP intervention if the CBD is normal and hence avoid the associated risk of ERCP (pancreatitis 4-20% and bleeding <5%).
|
Table 1: Defined indication of EUS evaluations |
|
|
Structures |
|
|
Mediastinum |
Staging of oesophageal tumour |
|
|
Staging of lung tumour |
|
|
Assessment of mediastinal lymph nodes or structures |
|
Stomach |
Local staging of gastric tumour |
|
|
EUS guided transgastric drainage of abscess, pancreatic necrosis, biopsy of liver, pancreas, adrenal or lymph nodes |
|
|
Evaluation of submucosal tumours/lesions (lipoma, leiomyoma, GIST, pancreatic rest cells, linnitus plastica etc...) |
| Pancreas |
Evaluation of pancreatic tumour, cysts or infective lesions (including FNA) |
|
Staging of pancreatic tumour |
|
|
Transgastric drainage of abscess or collections/necrosis |
|
| Hepatobiliary | Assessment of hepatic lesions especially in the left lobe |
| Assessment of the biliary tree especially the distal common bile (commonly difficulty to examine with transcutaneous US) | |
| EUS guided CBD cannulation and drainage | |
| Rectum | Local staging of rectal tumour |
| Assessment of rectal lesions: mucosal or submucosal | |
| EUS guided drainage of peri-rectal abscesses | |
| Prostate | Assessment/Staging of prostate carcinoma |
|
EUS guided prostate FNA |
|
Images prepared by Dr Chong Vui Heng, Consultant Gastroenterologist & Hepatologist, Department of Gastroenterology & Hepatology, RIPAS Hospital, Brunei Darussalam & Edited by Mr William Chong.
All images are copyrighted and property of RIPAS Hospital.
![]()