Figure 1
IMAGE OF THE WEEK
WEEK 22
|
|
|
|
|
Figure 1 |
|
TRACHEO-OESOPHAGEAL FISTULA
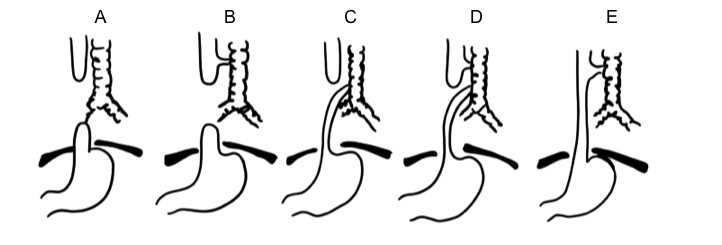
Tracheo-oesphageal fistula (TOF) is a congenital anomaly in which there is a connection between the oesphagus and the trachea, usually associated with a complete interruption of the proximal lumen of the oesphagus resulting in a blind upper-pouch. Figure 2 shows the various anatomical types with 85% of all cases are of type C TOF.
|
|
|
|
Figure 2: Anatomical types of Tracheo oesophageal fistula |
|
60% of cases are associated with maternal hydramnios, which is largely responsible for the high frequency of premature births. Clinical signs of TOF in a newly borned infant is excessive saliva from the mouth and consequently a high incidence of aspiration pneumonia. This is accentuated if the infant is fed, when milk accumulate in the upper pouch and spill into the trachea, causing the infant to cough during feeding or even become cyanotic.
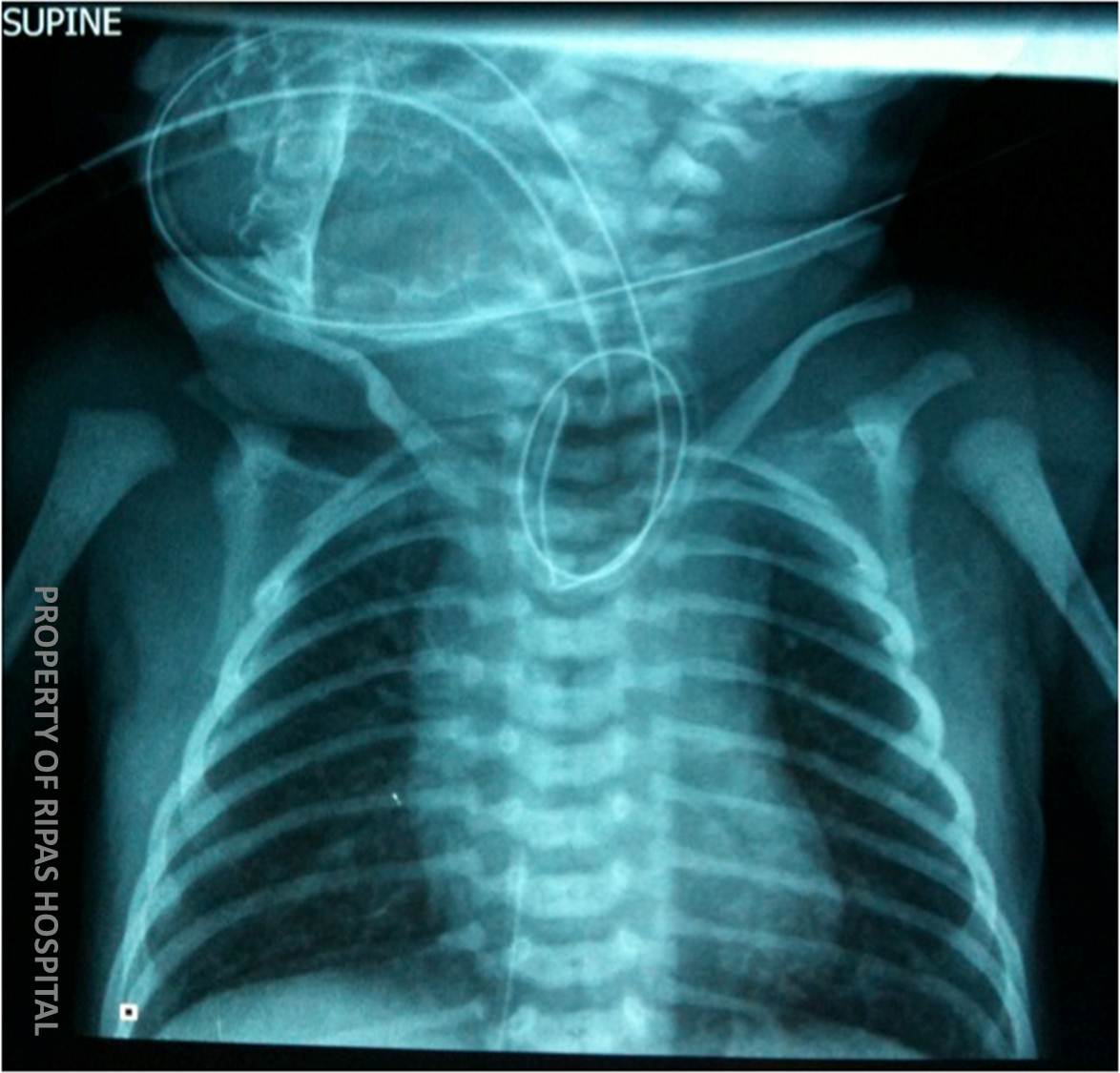
All infants should have a size 5 nasogastric tube passed down through the nostril into the stomach. If the NG tube fails to pass down into the stomach, a chest x-ray including the neck should be taken and if TOF is present, the nasogastric tube will get coiled up in the upper pouch as shown in Figure 1.
A baby with TOF should be nurse supine and propped up to 60º. Rehydration and correction of any electrolyte imbalance or hypoglycaemia is necessary before corrective surgery, which is the definitive therapy. Antibiotics will be required if there has been significant aspiration pneumonia. Prognosis for TOF is good with surgery but complications and sequelae from surgery are frequent.
Images prepared by Mr Chong Chee Fui, Consultant Cardiovascular & Thoracic Surgeon, Thoracic Unit, Department of General Surgery, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()