![]()
![]()
Figure 1a
Figure 1b
IMAGE OF THE WEEK
WEEK 25
|
|
|
|
|
Figure 1a |
Figure 1b |
|
AORTIC TRANSECTION
Aortic transection (Figure 1a) remains the second leading causes of death following road traffic accident (RTA), claiming 15% of RTA death, with 75-90% of cases died at the scene of the accident.
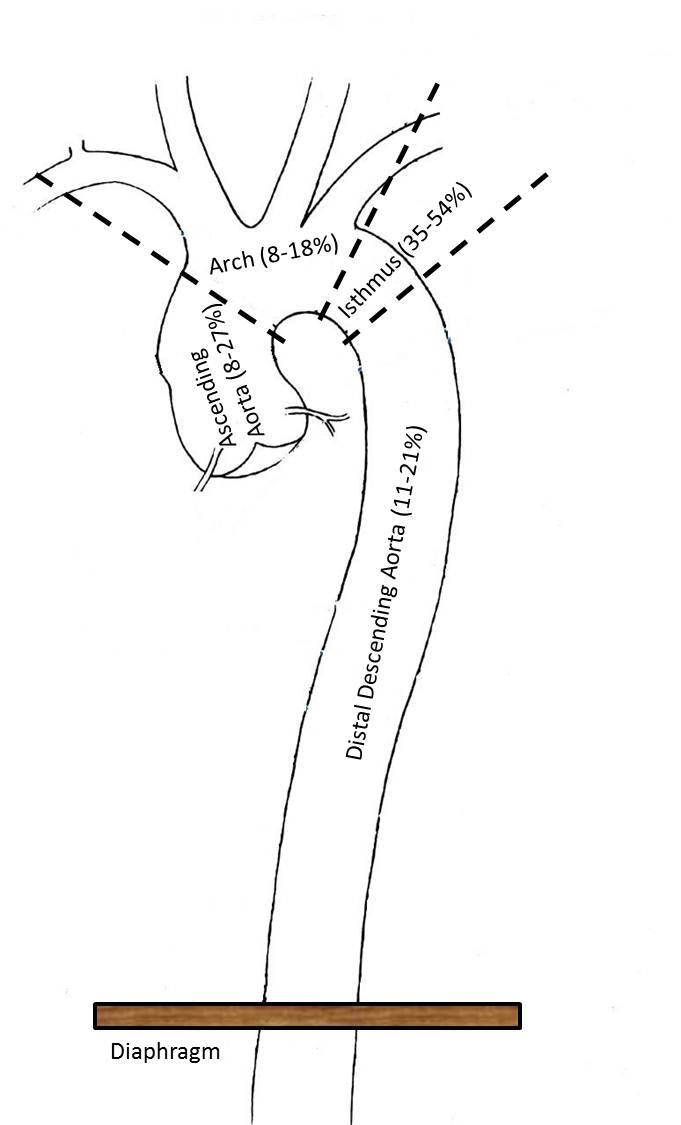
The mechanics behind aortic transection is the result of a sudden forward acceleration followed by sudden deceleration force associated with a head-on motor vehicle accident or a stationary pedestrian hit by a fast oncoming car, resulting in differential sliding displacement of two segments of the aorta, of which one of the segment is anchored or fixed by either branches or surrounding tissues or organs. Any segments of the aorta can be transected but the commonest site is the aortic isthmus (36-54%) [See figure 2]. The transection usually occurs in a transverse fashion involving all 3 layers.
|
|
|
Figure 2 |
For the few that survive to reach a hospital with Trauma care, rapid confirmation of a diagnosis of aortic transection makes a significant difference between survival and death of the patient. A contrasted thoracic and abdominal CT should be performed urgently upon arrival if an initial chest radiograph shows mediastinum widening. Other radiographic features that may suggest aortic transection is shown in table 1. The CT appearance of aortic transection or aortic dissection can be difficult to differentiate but the clue to the former lies in the history of significant acceleration and deceleration injury and a large amount of mediastinal haematoma with a left haemothorax (Figure 1b). Other CT features of aortic transection is shown in table 1.
Table 1: Radiological features of aortic transection.
|
Chest Radiograph |
CT Scan |
|
Widened mediastinum (>8.0cm) |
Wall thickening |
|
Mediastinum-to-chest width ratio >0.25 |
Extravasation of contrast (Figure 1) |
|
Tracheal shift to the patient’s right |
Filling Defects (Figure 1: Arrow) |
|
Blurred aortic contour |
Para-aortic Haematoma (figure 1: arrow head) |
|
Irregularity or loss of the aortic knob |
Intimal flaps/irregular intimal outline (Figure 1b) |
|
Left apical cap |
Mural thrombi |
|
Depression of the left main bronchus |
Pseudoaneurysms |
|
Opacification of the aortopulmonary window |
Pseudocoarctation |
|
Right deviation of the nasogastric tube |
Left haemathorax (Figure 1: star) |
|
Wide paraspinal lines |
Pocket of contrast outside of aortic lumen |
|
First rib fracture |
|
|
Any other rib fracture |
|
|
Clavicle fracture |
|
|
Pulmonary contusion |
|
|
Thoracic spine fracture |
|
Patients diagnosed with aortic transection requires to be referred urgently to a
cardiothoracic unit for emergency repair of the transected aorta either with an
open thoracotomy and replacement of the transected segment using a
Gortex or Dacron graft, or Thoracic Endovascular aortic repair (TEVAR) with
covered stented graft.
Images prepared by Mr Chong Chee Fui, Consultant Cardiovascular & Thoracic Surgeon, Thoracic Unit, Department of General Surgery, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()