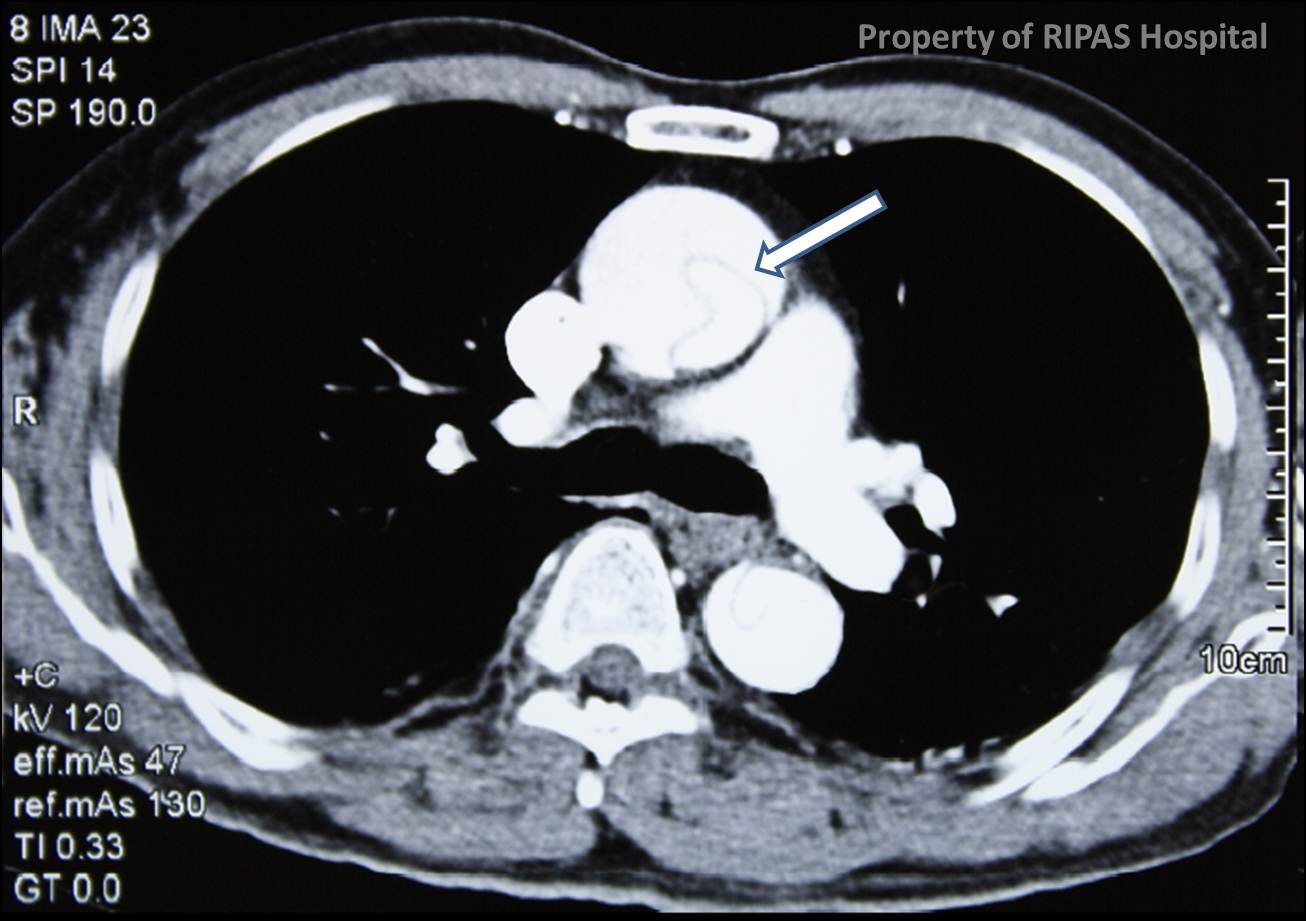
Figure 1a
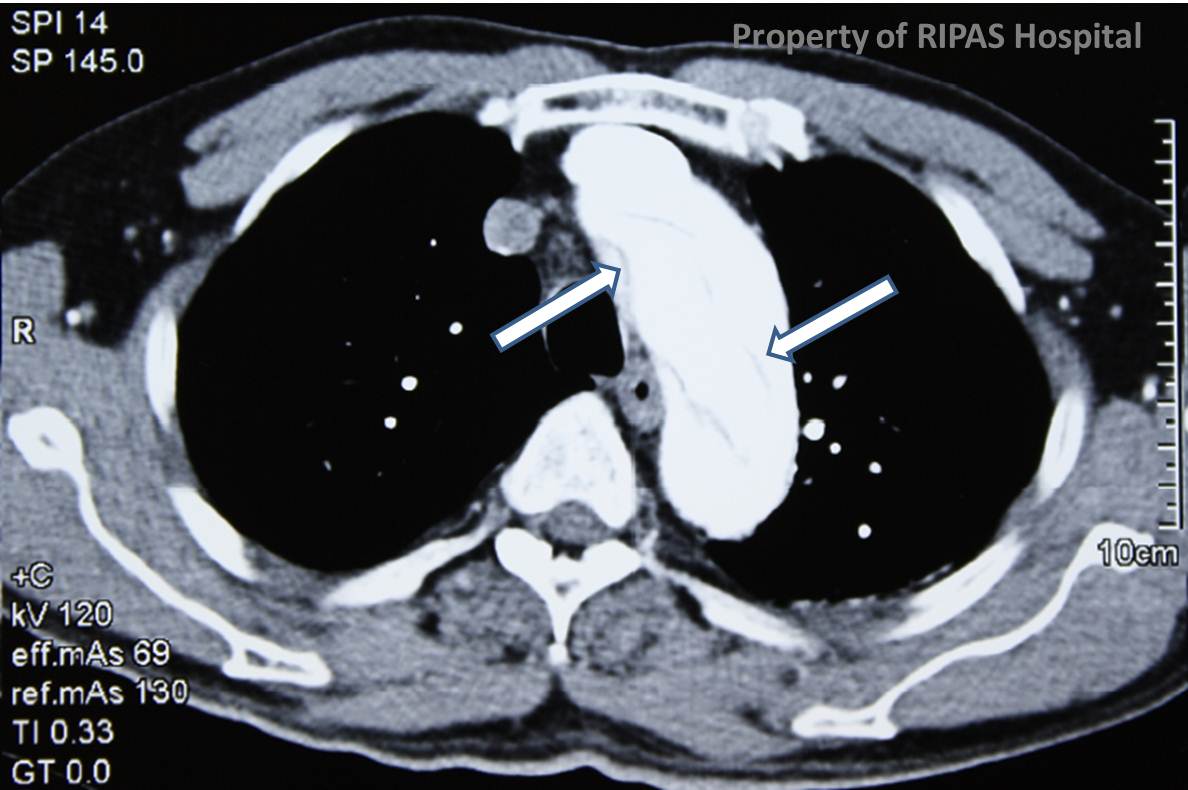
Figure 1b
liIMAGE OF THE WEEK
WEEK 27
|
|
|
|
|
Figure 1a |
Figure 1b |
|
AORTIC DISSECTION
Aortic dissection is a condition characterised by a tear in the intima of the aorta causing blood to flow between the media and the adventitia of the aorta, creating a false channel, as shown above in Figure 1 (White arrow pointing at a heart-shaped true channel, surrounded by a larger false channel, in the ascending thoracic aorta). Aortic dissection has an estimated worldwide annual prevalence of 0.5 to 2.95 per 100,000.
There are 2 systems of classification for describing aortic dissection as shown in the table 1.
| DEBAKEY CLASSIFICATION | STANFORD CLASSIFICATION |
DESCRIPTION |
| I | A | Origin of acute dissection flap found in the ascending thoracic aorta with false lumen extending through the entire length of the aorta. |
| II | Origin of acute dissection flap found in the ascending thoracic aorta with false lumen involving only the ascending aorta. | |
| III | B | Origin of acute dissection flap found in the descending thoracic aorta with false lumen involving only the descending thoracic aorta. |
| IV | Origin of acute dissection flap found in the descending thoracic aorta with false lumen involving the descending thoracic and abdominal aorta. |
There are also differences in terms of clinical characteristics of patients presenting with Type A or Type B aortic dissection (see linked).
There are several hypotheses postulated regarding the aetiology of intimal tear which permits blood under pressure to dissect down the plane between the media and adventitia. One such hypothesis is due to biochemical abnormality within the media, such as fibrillin abnormality found in patients with Marfan's syndrome. This group of patients have a high incidence of acute aortic dissection and should be suspected in cases of acute aortic dissection. Another hypothesis is one of intramural haematoma from a penetrating atherosclerotic ulcer or bleeding from vasa vasorum, creating a plane between the media and the adventitia as the primary event. The resulting intramural haematoma creates localised areas of increased stress in the intimal during diastole. With the primary events hypothesised above occurring, and in the presence of hypertension (usually present in over 75% of all cases of acute aortic dissection), intimal tears occurred and propagate down the dissection plane. In the current era of endovascular based intervention, intimal tear resulting in aortic dissection from catheter procedures is increasingly recognised as an iatrogenic caused. Although no single risk factor is responsible for aortic dissection, several risk factors have been identified (see linked).
Over 70-90% of patients present with the classic symptom of acute onset of sharp tearing chest pain which radiates to the back. Other symptoms include syncope (13%) and abdominal pain (22%). On clinical examination, hypertension is usually present in over 70% of patients. Limb pulses may be weak suggesting involvement in the dissection. Focal neurological signs suggest involvement of the carotids and the carotids should be auscultated for bruit. An early diastolic murmur at the left sternal edge may suggest aortic regurgitation from involvement of the aortic root.
Classic chest radiograph appearance suggesting aortic dissection is one of widened mediastinum, for which every junior doctors have been taught to look out for. A contrast CT of the aorta including the neck and down to the femorals should be obtained to confirm the diagnosis and assess the extend of the dissection (Figure 1). ECG should be obtained and any ischaemic changes may indicate coronary artery disease or dissection of the coronary ostial, in which case a coronary angiogram may be indicated. In patients with an aortic murmur, a TEE is indicated to assess the aortic root and the aortic valve.
For all aortic dissection involving the ascending aorta and arch, emergent surgery is indicated as mortality increases by 1% for every hour of delay. Pre-operative control of BP should be achieved using Labetolol infusion to maintain a systolic blood pressure below 120 mmHg. Patient with ascending aortic dissection should be referred urgently to a cardiothoracic surgeon. Patients with Stanford Type B descending thoracic aortic dissection should be treated conservatively with BP control. Surgery is only indicated for extension of dissection with end organ ischaemia such as mesenteric or renal ischaemia, usually presented as continuing pain despite BP control. Endovascular aortic stenting is now commonly employed as first line for Stanford Type B aortic dissection.
Images contributed by Mr Chong Chee Fui, Department of General Surgery (Thoracic Unit), RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()