IMAGE OF THE WEEK
WEEK 29
|
|
|
|
|
|
|
|
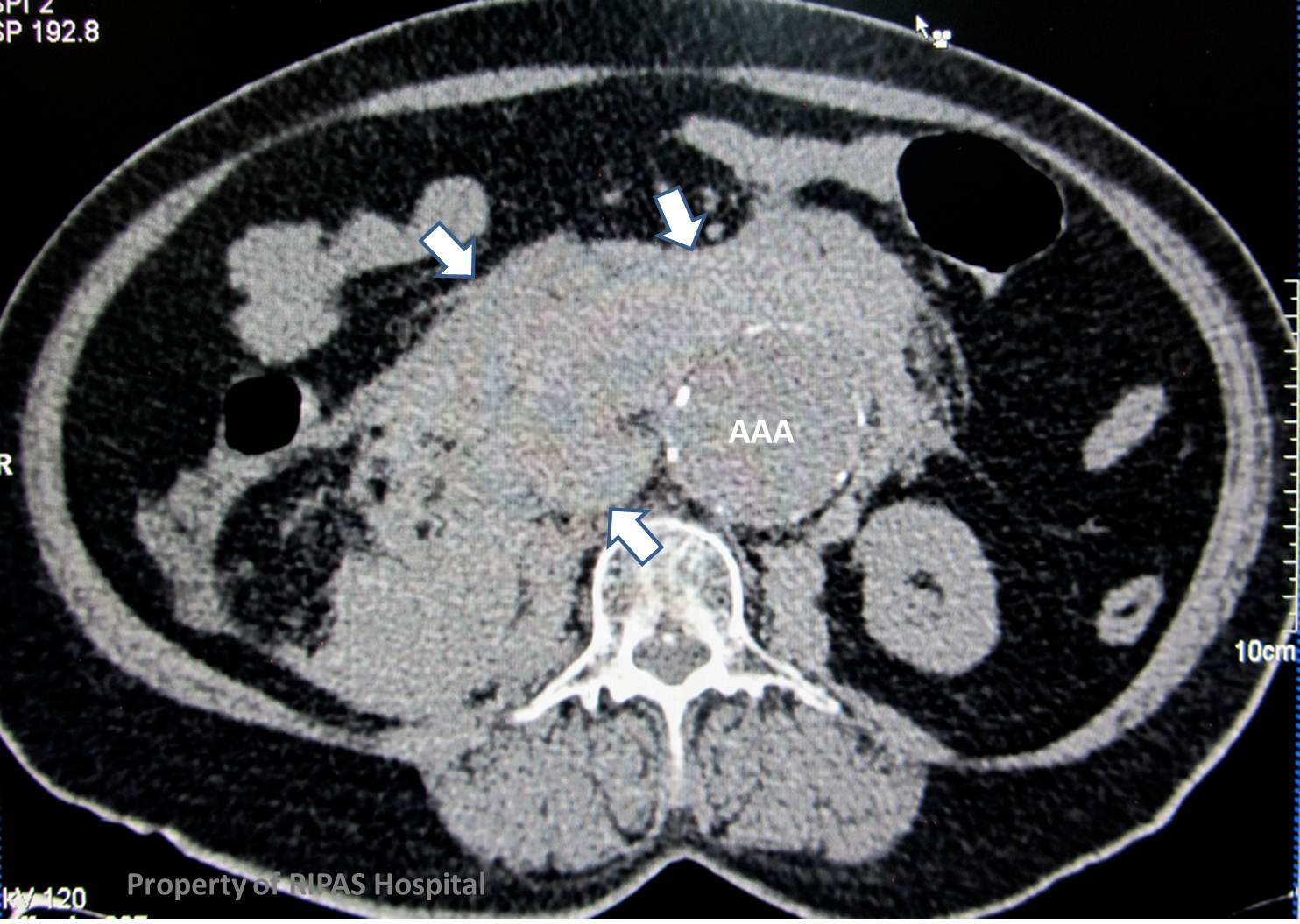
ABDOMINAL AORTIC ANEURYSM
Enlargement of the diameter of the abdominal aorta, greater than 3cm is considered aneurysmal.
Size is closely related to the risk of rupture, with those measuring less than 4cm having a virtual 0% risk versus 20% for those greater than 6cm.
Know asymptomatic aneurysms are followed with surveillance ultrasound. Those being considered for elective treatment, either surgically or by endovascular stenting, require a pre-operative planning CT to assess for aneurysmal characteristics.
In the acute setting, there is only one choice – CT and FAST.
A non-contrast scan is virtually always sufficient to detect a rupture, and delay whilst performing a contrast study will delay the patient getting to theatre, where their life can be saved, not on the CT scanner table.
In addition to identifying the aneurysm size and location (supra, juxta or infra-renal), acute blood in the form of high attenuation material in the retroperitoneum, indicates rupture.
TREATMENT
In cases of leaking or contained ruptured AAA (as in the above case), emergent surgery to replace the abdominal aorta is the treatment of choice but carries significant intra-operative and 30-day mortality of 6.1% and 45.5% respectively. Emergent endovascular aortic stent replacement or EVAR is becoming increasingly popular for emergent treatment of leaking or ruptured AAA as it carries less peri-procedural and 30-day mortality of 4% and 20% respectively. However, a recent study of aneurysm related mortality rates in the US AneuRx Clinical trial published in the J Am Coll Surg 2010 indicated that long-term mortality of patients implanted with the AneuRx (Metronic) graft probably exceeds those treated with open surgery within 4 years of implant.
Images contributed by Dr Ian Bickle, Department of Radiology, RIPAS Hospital, Brunei Darussalam and edited by Mr William Chong.
All images are copyrighted and property of RIPAS Hospital.
![]()