Figure 1: Click on image to enlarge
IMAGE OF THE WEEK 2012
WEEK 3
PECTUS EXCAVATUM
|
|
|
|
|
Figure 1: Click on image to enlarge |
|
|
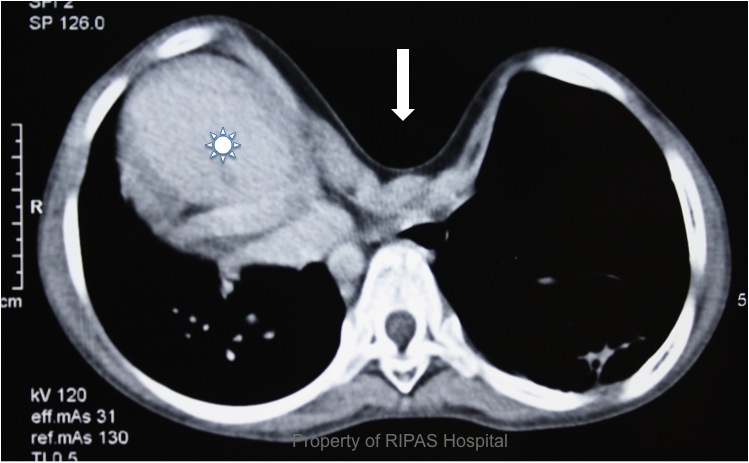
Pectus excavatum (PE) is an abnormal development of the anterior rib cage resulting in sunken depression of the sternum (breastbone), often referred to as ‘funnel chest’ or ‘sunken chest’(Figure 1). This deformity is often present at birth which can be mild or severe but progresses as the child grows, reaching maximum depression by teenage years as bone growth stops.
The cause of PE is not well understood but there are evidence to indicate that the underlying abnormality may be due to hyperplasia of the affected costal cartilages or an inmmaturity of the developing costal cartilages, due to failure of sulfation of the proteo-glycans matrix with a cross-linked sulphur molecule to the collagen fibers, making the cartilage matures and increasing its strength. This immature cartilage is softer in texture making it easy to bend and flex to the stresses associated with growing bone and cartilage.
Most patients do not complained of any significant symptoms and presents to medical attention with psychosocial problems. However, if the depression is as severe as in this case (Figure 1: white sun label), with displacement of the heart to the right, cardiorespiratory symptoms may be present. In severe cases of PE, patients usually have reduced exercise capacity with easy fatique on mild exercises, shortness of breath and even chest pain. There may also be an abnormal restrictive pattern of airway obstruction on spirometry. Other associated cardiac abnormalities may include mitral valve prolapse and regurgitation, arrhythmias, aortic regurgitation, ASD, Tetralogy of Fallot, dextrocardia, tricuspid regurgitation, PDA etc.
PE is the most common types of congenital chestwall deformity, accounting for approximately 90% of all congenital chestwall deformities. PE occurs more often in men than women, with an incidence of 1 per 300 to 400 white male births. Other associated musculoskeletal disorders include scoliosis, Marfan’s syndrome, Pierre Robin Syndrome, Prune-belly syndrome, neurofibromatosis, Tuberous sclerosis and congenital hernia.
PE is not preventable but the condition is easily treatable surgically. Management of PE has always been thought of as a comestic procedure but in the more recent decades, corrective procedures are more often done for medical reasons.
Before pectus excavatum can be properly treated, it must first be properly diagnosed. Your doctor and other specialists, including a thoracic surgeon and pulmonologist, will perform a complete physical exam and comprehensive blood tests to confirm the diagnosis.
Several other tests may be performed, including
• Physical (stress) test
• Pulmonary function test
• Laboratory studies (blood work), such as chromosome studies or enzyme assays
• Metabolic studies
• Chest x-ray
• Computed tomography (CT) scan of the chest
• Electrocardiogram (EKG)
• Echocardiogram (a picture of the heart)
Currently the most common corrective procedure performed for PE is the minimally invasive Repair of Pectus excavatum, ‘MIRPE’ in short or also know as the ‘NUSS procedure’ after Professor Donald NUSS, the paediatric surgeon who developed the technique. This procedure involves introducing a stainless steel or titanium bar, which has been pre-bend to correct the sunken depression into the thoracic cavity via 2 slit incisions on the lateral chest wall, under the sternum and across to the other pleural space using thoracoscopy. This bar is then rotated with the convex side facing anteriorly under the sternum, hence correcting the deformity. A small steel grooved plate may be attached to the ends of the bar to stabilize the bar and prevent rotation or up and down movements, which may result in displacement of the bar later on.
|
|
|
|
|
Figure 2a: Preop |
Figure 2b: Postop |
|
Figure 2 shows the PE deformity before and after MIRPE procedure.
The stainless bar is left for 2-3 years to allow for the chest wall to remodel to a more normal shape before it is removed, 2 years after implantation. The benefit of this procedure is less pain due to the minimally invasive technique, shorter hospital stay and more rapid recovery and return to work or school as in this case.
Prior to the introduction of the MIRPE procedure, PE were corrected using an extensive subperichondrial excision of all abnormal deformed cartilages, the sternum was split superiorly in order to elevate the depressed sternum. This procedure, known as the Ravitch procedure involves significant dissection and tissue trauma, resulting in significant pain, haematoma formation and infection. The most severe form of complication associated with the Ravitch procedure, particularly if the procedure was performed in early childhood and if significant amount of costal cartilages have been removed, is a narrow deformity of the rib case at the diaphragm level due to failure of growth of the lower rib cage, a condition known as asphyxiating osteodystrophy.
Image and text contributed and prepared by
Mr Chee Fui Chong, Thoracic Unit, Department of Surgery, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()

