Figure 1
IMAGE OF THE WEEK
WEEK 38
OESPHAGEAL CANDIDIASIS OR THRUSH
|
|
|
|
|
Figure 1 |
|
|
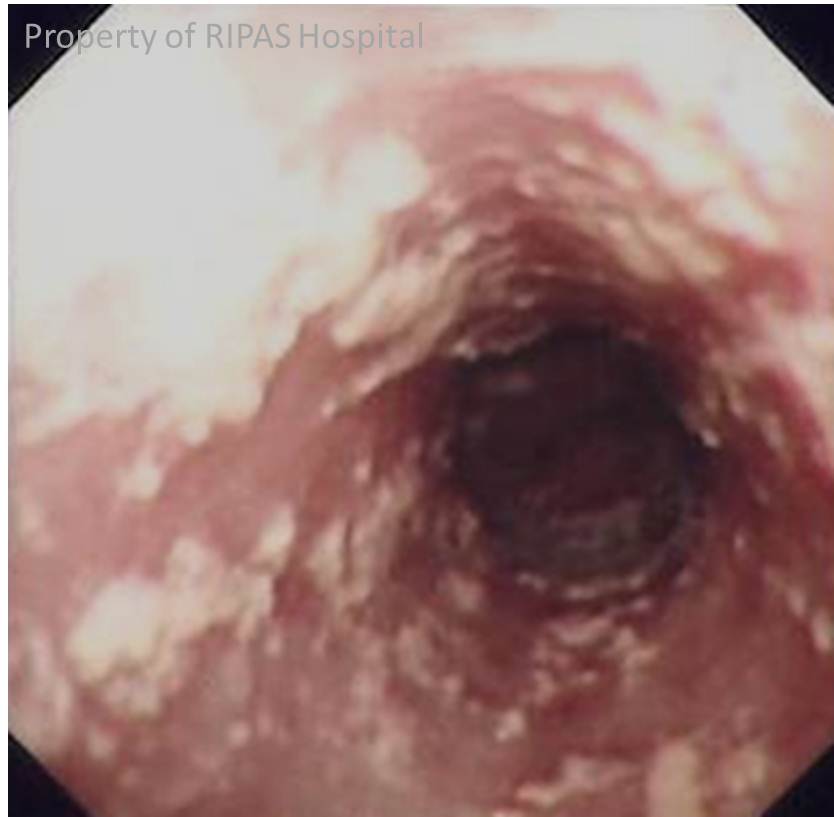
The endoscopic image (Figure 1) shows multiple whitish patches in the oesophagus due to oesophageal candidiasis.
Candidiasis or thrush refers to infections caused by fungus or yeast, Candida species, of which Candida albicans (C. albicans) is the most common. It is also referred to as candidosis, moniliasis and oidomycosis. C. albicans is previously referred to as Monilia albicans and Oidium albicans, hence the term moniliasis and oidomycosis.
Candida yeasts are commonly present in human as commensal organism (including oral cavities and the intestine) and their growth is control by the host immune system and also by the other commensal bacteria. Once this balance is disturbed, Candida species can proliferate resulting in clinically significant manifestations.
C. albican can cause infection of almost every organ but certain structures are more commonly affected. Candidiasis encompasses infections that range from the more common superficial structures such as oral thrush, vaginitis and oesophageal candidiasis to the life threatening systemic infections, candidemia which usually occur in severely immune compromised patients: transplantations, cancers, post chemotherapy and AIDS. However, even patients without these risk factors can be affected with disseminated candidemia.
Superficial infections of mucosal membranes such as oral thrush and oesophageal candidiasis results in local inflammation resulting in discomfort: odynophagia and dysphagia. However most do not have any oropharyngeal or oesophageal complaints. Oral thrush or oesophageal candidiasis appears as white discrete patches that can be scrapped off leaving slightly inflamed base. In patients with AID, candidiasis may be found along with other infections such as Herpes simplex or CMV oesophagitis. Apart from risk factors mentioned above, other risk factors for oesophageal candidiasis include steroid therapy (including steroid inhalers), acid suppressions, recent antibiotic use, underlying diabetes mellitus (usually poorly controlled) and nutrient deficiencies.
Candidiasis can be treated by removing the precipitating factors (i.e. acid suppression and antibiotic use) and use of antifungal drugs that can be topical (cream, suppository or douches), oral or intravenous. Mild infections can be treated with oral or topical antifungal such as clotrimazole, fluconazole, ketoconazole and nystatin where severe infections may require more potent (more toxic) antifungal (amphotericin B, caspofungin or variconazole). For oesophageal candidiasis, a 7 to 10 days course of fluconazole (100 mg daily) is usually adequate.
Images contributed and prepared by
Dr Chong Vui Heng, Specialist Gastroenterologist, RIPAS Hospital, Brunei
.
All images are copyrighted and property of RIPAS Hospital.
![]()