Figure 1: Click on image to enlarge.
IMAGE OF THE WEEK
WEEK 40
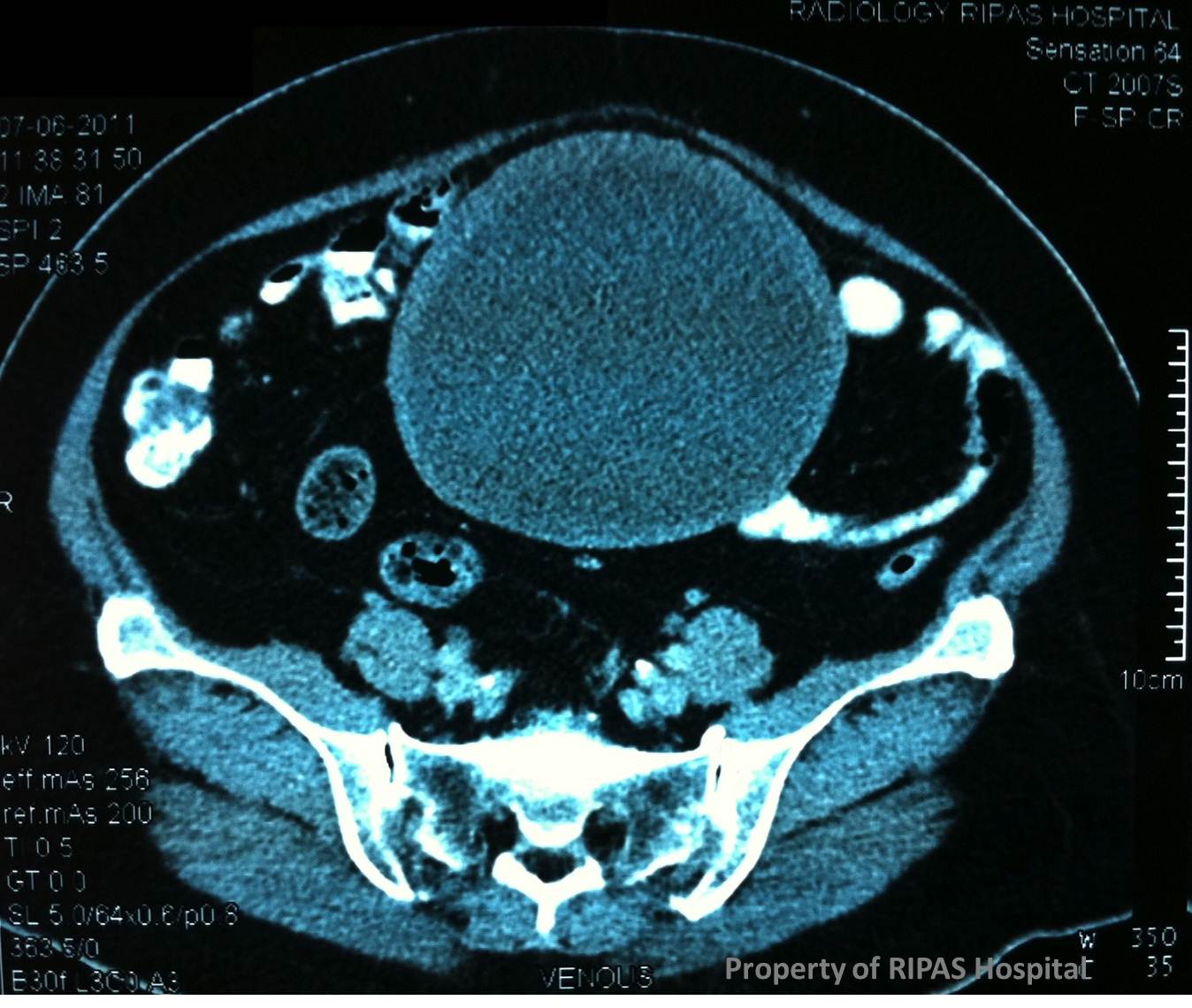
MESENTERIC OR OMENTAL CYST
|
|
|
|
|
Figure 1: Click on image to enlarge. |
|
|
Mesenteric and omental cysts are rare with an incidence of about 1 in 140,000 general hospital admissions and about 1 in20,000 pediatric hospital admissions. Approximately one third of cases occurred in children under 15 years of age. The condition was first described by an Italian anatomist Benevieni following an autopsy on an 8-year-old girl.
Mesenteric and omental cysts benign conditions resulting from the proliferations of ectopic lymphatics that lack communication with normal lymphatic system and are thought to arise from lymphatic spaces associated with embryonic retroperitoneal lymphatic sac, analogous to cystic hygroma. Other aetiologies include lymphatic obstruction secondary to trauma, neoplasm or failure of leaflets of mesenteric to fuse or embryonic lymphatics to connect to the venous system and degeneration of lymph nodes.
Mesenteric cyst can be simple as shown in figure 1 above or multiple, unilocular (figure 1) or multilocular and may contained haemorrhagic, serous (ileal and colonic cysts), chylous (jejunal cysts) or infected fluid. Size can vary from a few millimetres to as large as 40cm (the one in figure 1 is about 10cm).
Mesenteric cysts can present as incidental findings on laparotomy or as in this case abdominal pain with increasing distension and a palpable mass.
Mesenteric cysts on plain abdominal x-ray appear as a gasless, homogeneous, water-dense mass that displaces the bowel loops laterally or anteriorly. There may be calcification on the wall of the cyst. Ultrasound examination will revealed a cystic lesion with thin septa and sometimes with internal echoes characteristics of debris, haemorrhagic fluid or infection. It is the investigative modality of choice. CT abdomen as in this case, may exclude cysts arising from other abdominal structures such as kidney, pancreas or ovary.
Incidental findings or mesenteric cysts or symptomatic mesenteric cysts should be removed surgically by enucleation or completed removal with surrounding rim mesenteric. If removal is not possible, then marsupialization can be performed but should be followed by sclerosing of the cyst lining with 10% glucose solution.
Overall surgical results is satisfactory with recurrence rate ranging from 0 – 13.6%, averaging about 6.1% in a series of 162 adults and children.
Images contributed and prepared by
Mr CF Chong, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()