Figure 1: Click on image to enlarge.
IMAGE OF THE WEEK
WEEK 43
CHYLOTHORAX
|
|
|
|
|
Figure 1: Click on image to enlarge. |
|
Chylothorax is a condition characterised by the presence of a thick milk-liked fluid in the pleura cavity, most typically on the left side (Figure 1). This usually occurs as a result of a tear or disruption of the thoracic duct resulting in leakage of chyle into the pleura space. The amount can be huge since the thoracic duct transport up to 4L/day of chyle in a normal adult.
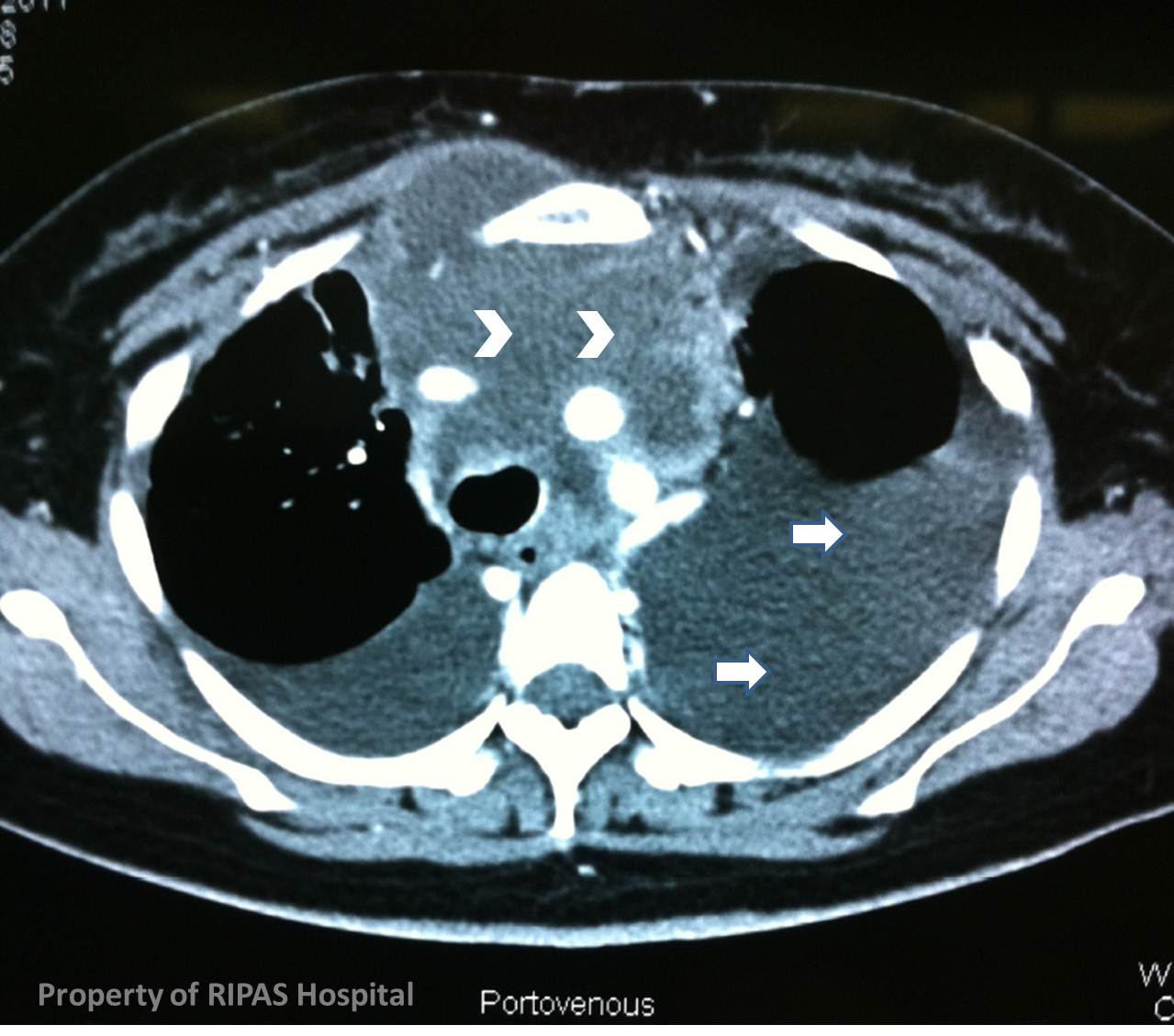
Common causes can be categorised into malignant and non-malignant aetiologies. Most common malignant aetiology is an anterior mediastinal malignancies (50% of cases) such as lymphoma as in this case, which accounts for 60% of cases (Figure 2: arrow heads). Other malignant causes include pancoast tumour of the lung. Non-malignant causes include tuberculosis, sarcoidosis, cirrhosis, amyloidosis, filariasis and trauma. The incidence of chylothorax after cardiothoracic surgeries is about 0.2-1% due to the traumatic disruption of the thoracic duct during dissection of the mediastinum. In children, it can accounts for as much as 69-85% of all cases following cardiac surgeries. Congenital chylothorax accounts for the leading cause of pleural effusion in neonates.
|
|
|
|
Figure 2a: Click on image to enlarge. |
Figure 2b: Click on image to enlarge. |
Patients usually present with the classical symptoms of a large pleural effusion (Figure 2: arrows), which are increasing shortness of breath and tachypnoea with signs of reduced breath sounds, shifting dullness on the affected sides and tracheal deviation to the non-affected side if the effusion is large.
Diagnosis is rapid and simple with a biochemical analysis of the pleural fluid for triglyceride levels:
|
Triglyceride levels |
Diagnosis |
|
> 110mg/dL (> 1.25mmol/L) |
99% certainty that the fluid is chyle. |
|
50-110mg/dL (0.6-1.25mmol/L) |
use lipoprotein analysis to inspect the pleural fluid for chylomicrons or cholesterol crystals. |
|
< 50mg/dL (<0.6 mmol/L) |
5% certainty that the fluid is chyle |
|
A ratio of pleural fluid cholesterol to triglyceride of less than 1 is also diagnostic. |
|
In this case, the patient’s pleural fluid triglyceride level was 11.22 mmol/L, which is diagnostic of chylothorax. In the initial aspiration of the pleural fluid, it can be easily mistaken for pus and sent for culture which is usually sterile due to the high contained of lymphocytes and antibody titres in the fluid.
Imaging usually confirmed a large effusion (Figure 2: arrows) with possible cause of the effusion as in this case a large anterior mediastinal Hodgkin’s lymphoma (Figure 2: arrow heads) which has disrupted the thoracic duct in the left anterior mediastinum (Figure 2b).
Treatment include immediate thoracostomy and drainage for symptomatic relief. Conservative measures include putting the patient on a fat free diet or on middle chain triglycerides diet or complete parenteral nutrition, to reduce the load through the thoracic duct. Chemoradiation may promote resolution of chylothorax and should be used in patients with malignant chylothorax who are not surgical candidates. Somatostatin (3.5-12 mcg/kg/hr) and its analogue octreotide has been used successfully in a number of paediatric cases of chylothorax following surgery or other iatrogenic causes, but complications of somatostatin therapy such as diarrhoea, hypoglyceamia and hypotension limits its used. All these conservative therapy will take time to work and patient should be told of the protracted time of treatment which can take up to 2 weeks.
Patient who failed medical therapy should be referred for surgical option of right VATS ligation of thoracic duct which is successful in 100% of the time if the thoracic duct is completedly ligated and divided. To ease the location and identification of the thoracic duct, patient should be given 60-90mls of cream or full cream milk mixed with 1% methylene blue enterally via an NG tube 30-60 minutes prior to incision. The procedure can be performed using right VATS via 3-4 ports and after opening the pleura inferior to the inferior pulmonary vein, the thoracic duct can be located between the azygos vein and oesophagus. A long segment should be dissected out and ligaclipped. The thoracic duct should then be divided and the ends reflected back and ligaclipped to the rest of the remaining thoracic duct. The effect is almost immediate with reduce production of chyle in the left chest drain which is obvious the next day after a normal diet.
Image and text contributed and prepared by
Mr William Chong, Department of General Surgery, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()