IMAGE OF THE WEEK 2013
WEEK 5
MANAGEMENT OF DISLODGED
PORT-A-CATHETER
|
 |
|
|
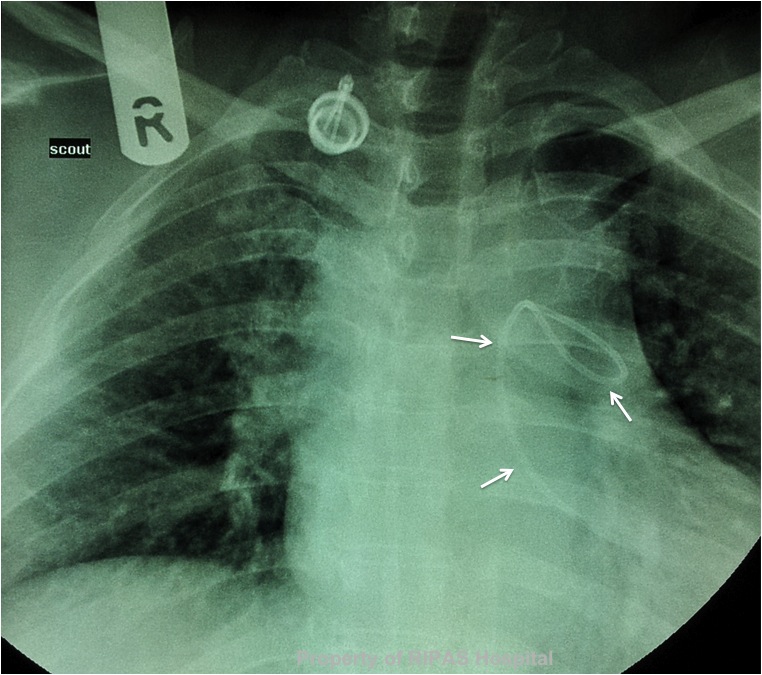
Figure 1: Dislodged port-a-catheter as
indicated by the catheter (white arrows) which is found in the right
ventricle and left pulmonary artery. It is no longer connected to the
port which is found in the right anterior chest wall.
(Click on image to
enlarge) |
|
Dislodgement of port-a-catheter is an uncommon event, with a
reported incidence of about 4.1% to 5.1%.
(1,2)
In a reported series, 42% of the dislodged catheter ended up in the right
ventricle, 33% in the right atrium and 25% in the pulmonary artery. Figure 1
showed a dislodged port-a-catheter, completely disconnected from the main port
in the right anterior chest wall with the proximal end of the catheter resting
in the right ventricle and the distal end looping in the left pulmonary artery.
In 80% of the cases, the patients presented with port-a-catheter
dysfunction and dislodgement confirmed on chest x-rays. In the remaining 20%,
the dislodgement were diagnosed at surgical removal.
Possible mechanism by which dislodgement occurs may be due to
degradation of the catheter material over time, which results in most cases to
fracture of the catheter rather than dislodgement. Over zealous flushing of
port-a-catheter, particularly if the catheter is occluded may result in
stretching and ballooning of the catheter over the snout of the connector of the
port and thus dislodgement. In the case depicted in Figure 1, the patient
reported several months back, feeling a sharp pain with swelling around the port
when the nurse forcefully flushed her port-a-catheter during a follow-up visit.
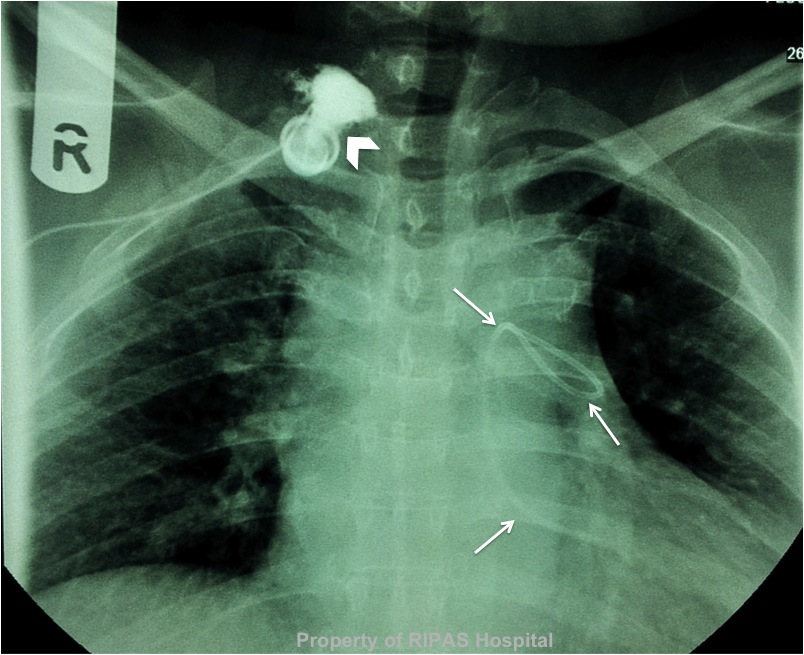
The dislodgement occurred a while back as instillation of contrast into the
port, showed extravasation of contrast into the surround subcutaneous tissue and
not into the vein (Figure 2). The tract between the right internal jugular vein
and the port would have sealed off by then.
|
 |
|
Figure 2: Instillation of contrast into the
port resulted in extravasation of the contrast into the surrounding
subcutaneous tissue (white arrow head). The tract between the right
internal jugular vein and the port has completely sealed over.
(Click on image to
enlarge) |
To date, there are very little or no reports of complications
arising from a dislodged catheter, mainly because most of the dislodged or
fracture catheters are removed immediately once they are diagnosed. However,
complications that can arise are related to infection of the catheter,
thrombosis and embolisation or it can migrate further down the pulmonary artery
causing pulmonary embolism of the distal segment of the lung supplied by the
occluded pulmonary artery.
Management of dislodged port-a-cath is usually non-surgical via
transcatheter techniques using a gooseneck snare guidewire under fluoroscopic
guidance in 98%-100% of cases. The catheter is easily removed without
significant complications. Open surgical removal is reserved for failed
percutaneous transcatheter removal and depending on the site at which the
catheter comes to rest, cardiopulmonary bypass may be required. The port is
removed surgically under local anaesthetic.
REFERENCES
1. Coccaro M, Bochicchio AM, Capobianco AM, Di Leo P,
Mancino G, Cammarota A. Long-term infusional systems: complications in cancer
patients. Tumori. 2001 Oct;87(5):308–11.
2. Ho C-L, Chou C-M, Chang T-K, Jan S-L, Lin M-C, Fu Y-C.
Dislodgment of port-a-cath catheters in children. Pediatr Neonatol. 2008
Oct;49(5):179–82.
Images and text contributed and prepared by
Mr William Chong, Thoracic Unit, Department of Surgery, RIPAS Hospital.
All
images are copyrighted and property of RIPAS Hospital.
