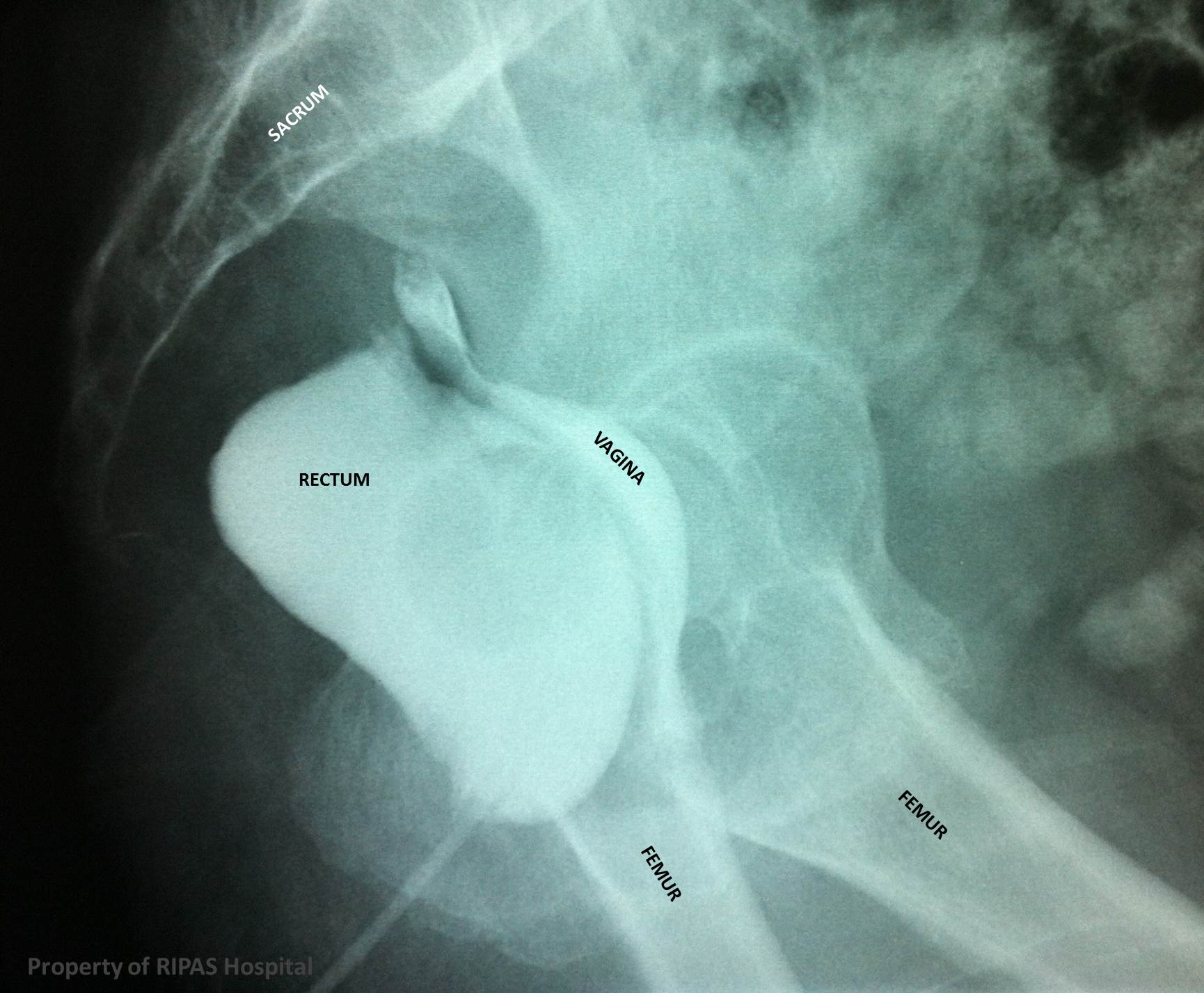
Figure 1: Barium enema showing contrast both in the rectum and vagina indicating a rectovaginal fistula. The fistula connection is not visible on this barium enema.
(Click on image to enlarge)
IMAGE OF THE WEEK 2013
WEEK 6
RECTOVAGINAL FISTULA
|
|
|
|
Figure 1: Barium enema showing contrast both in the rectum and vagina indicating a rectovaginal fistula. The fistula connection is not visible on this barium enema. (Click on image to enlarge) |
A rectovaginal fistula (RVF) is a connection or tract between the vagina and the rectum, which is lined by epithelium. RVFs are found just above the dentate line and are classified into 1) High – between the middle third of the rectum and the posterior vaginal fornix, 2) Low – between the lower third of the rectum and the lower half of the vagina.
The most common aetiology of acquired RVF is obstetric trauma, such as perineal laceration (episioproctotomy) during childbirth, particularly in primigravida, in precipitious birth or when vacuum or forceps extraction is used. Other causes include radiation injury (for pelvic malignancies, usually developed between 6 months and 2 years after completion of radiotherapy), infection (perirectal abscess/diverticulitis), inflammatory bowel disease (IBD - most often Crohn disease), operative trauma (stapled haemorrhoidopexy and Stapled transanal rectal resection [STARR] and transanal stapled resection [TRANSTAR]) and neoplasm.
Most patients with RVF present with passing flatus and faeces through the vagina, with frequent episodes of vaginitis and cystitis, which is understandably distressing.
Radiological studies such as barium enema (as shown in Figure 1) is the gold standard, which will demonstrate the fistula connection between the vagina and rectum. CT scanning often demonstrate perifistula inflammation between the vagina and part of the digestive tract, most commonly the rectum (Figure 2). Colonoscopy should be carried out prior to surgical correction to exclude inflammatory bowel disease by taking biopsies of the area. The biopsies will also exclude neoplastic aetiologies.
|
|
 |
|
Figure 2a: CT Barium enema (saggital plane) showing contrast both in the rectum and vagina indicating a rectovaginal fistula. (Click on image to enlarge) |
Figure 2a: CT Barium enema (transverse plane) showing contrast both in the rectum and vagina indicating a rectovaginal fistula. (Click on image to enlarge) |
Medical therapy includes local care, drainage of abscesses and antibiotic therapy in the acute episode. Dietary modification and supplemental fiber can reduce the discharge or symptoms during this period. With this therapy, most RVFs resulting from obstetric or operative trauma can heal completely. For patients with RVF secondary to Crohn disease, aggressive treatment with steroids, 6-mercaptopurine or azathioprine may help to control the primary disease allowing for surgical repair of the RVFs.
Surgical repair can be performed via a local approach for low RVFs or transabdominal approach for high RVFs. Local approach include techniques such as Transanal advancement flap repair, Transvaginal inversion repair, Bioprosthetic repair, Conversion to complete perineal laceration with layer closure and Simple fistulotomy. Transabdominal approach for high RVFs will include Fistula resection and closure with or without bowel resection and Ancillary procedures such as Bulbocavernosus flap and a variety of muscle, fascial and musculocutaneous flaps for repair of larger pelvic defect.
Images and text contributed and prepared by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
Mr William Chong, Thoracic Unit, Department of Surgery, RIPAS Hospital.
All images are copyrighted and property of RIPAS Hospital.
![]()
