Figure 1: Click on image to enlarge
IMAGE OF THE WEEK 2012
WEEK 6
ORBITAL CELLULITIS - SUBPERIOSTEAL COLLECTION
|
|
|
|
|
Figure 1: Click on image to enlarge |
|
|
Orbital cellulitis with the development of a subperiosteal collection is a true paediatric surgical emergency. Prompt treatment prevents blindness and other complications.
Orbital cellulitis in children is common and is typically caused by bacteria. The vast majority of cases are associated with acute sinusitis. Ethmoidal sinusitis is the most common source of orbital infection, due to its anatomical proximity to the orbit. The medial wall of the orbit is formed by the very ‘paper thin’ lamina papyracea, which separates it from the ethmoid sinuses and therefore is relatively easily disrupted with consequential intra-orbital extension.
The lamina papyracea, is perforated by nerves and blood vessels. This facilitates the communication of the organisms from the ethmoidal air cells into the subperiosteal space. For this reason the medial orbit is the most common site for an orbital abscess.
In orbital infections, the most common bacteria isolated are; Haemophilus influenzae, Staphylococcus aureus, Streptococcus pyogenes, Staphylococcus epidermidis, Streptococcus pneumoniae, and group A Streptococcus.
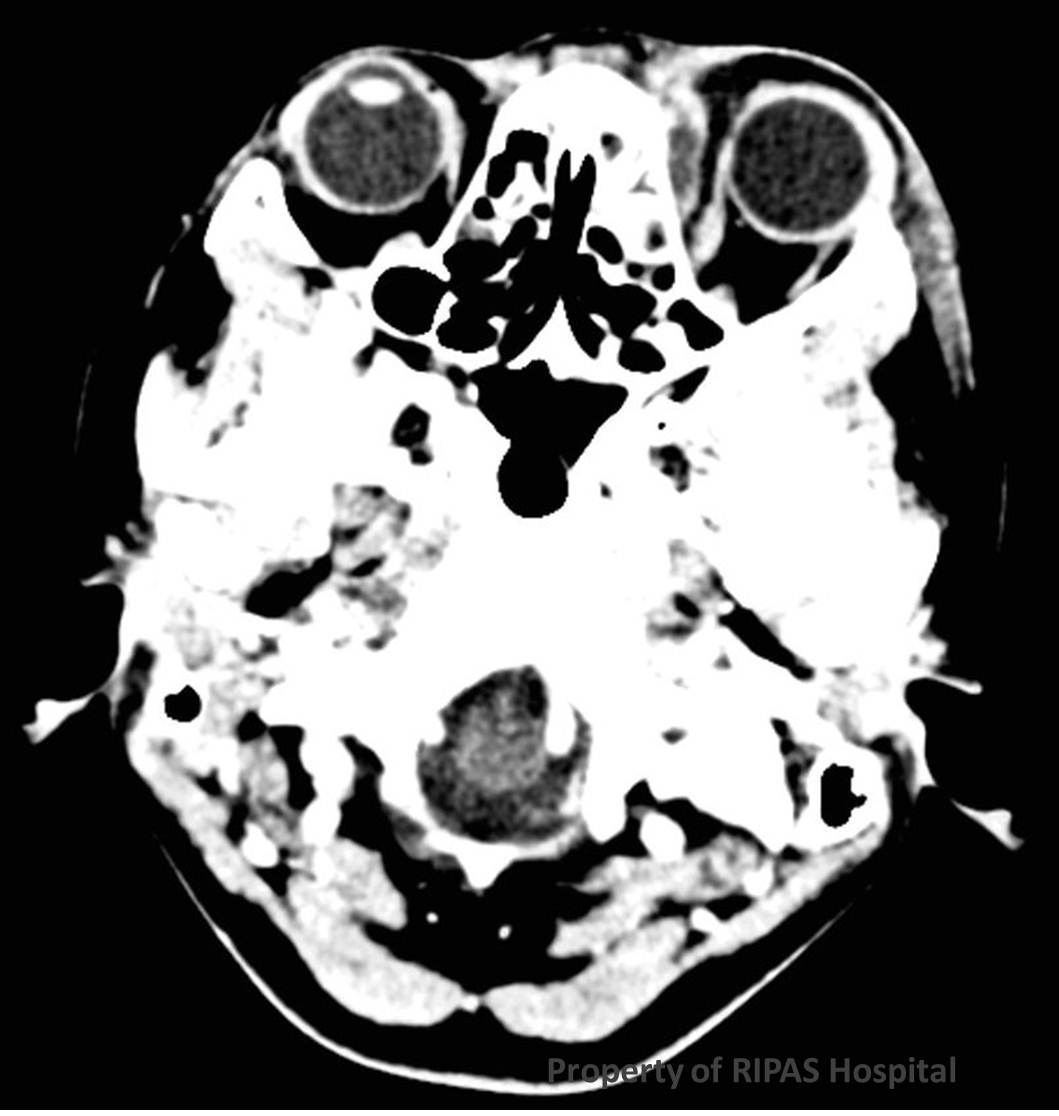
Urgent computed tomography (CT) of the orbits is indicated. The scanning range should be extended to include the para-nasal sinuses and the brain. The orbits are imaged both with and without contrast. The brain is imaged post contrast. This allows for the detection of complications, such as superior orbital vein or cavernous sinus thrombosis and intracranial abscess.
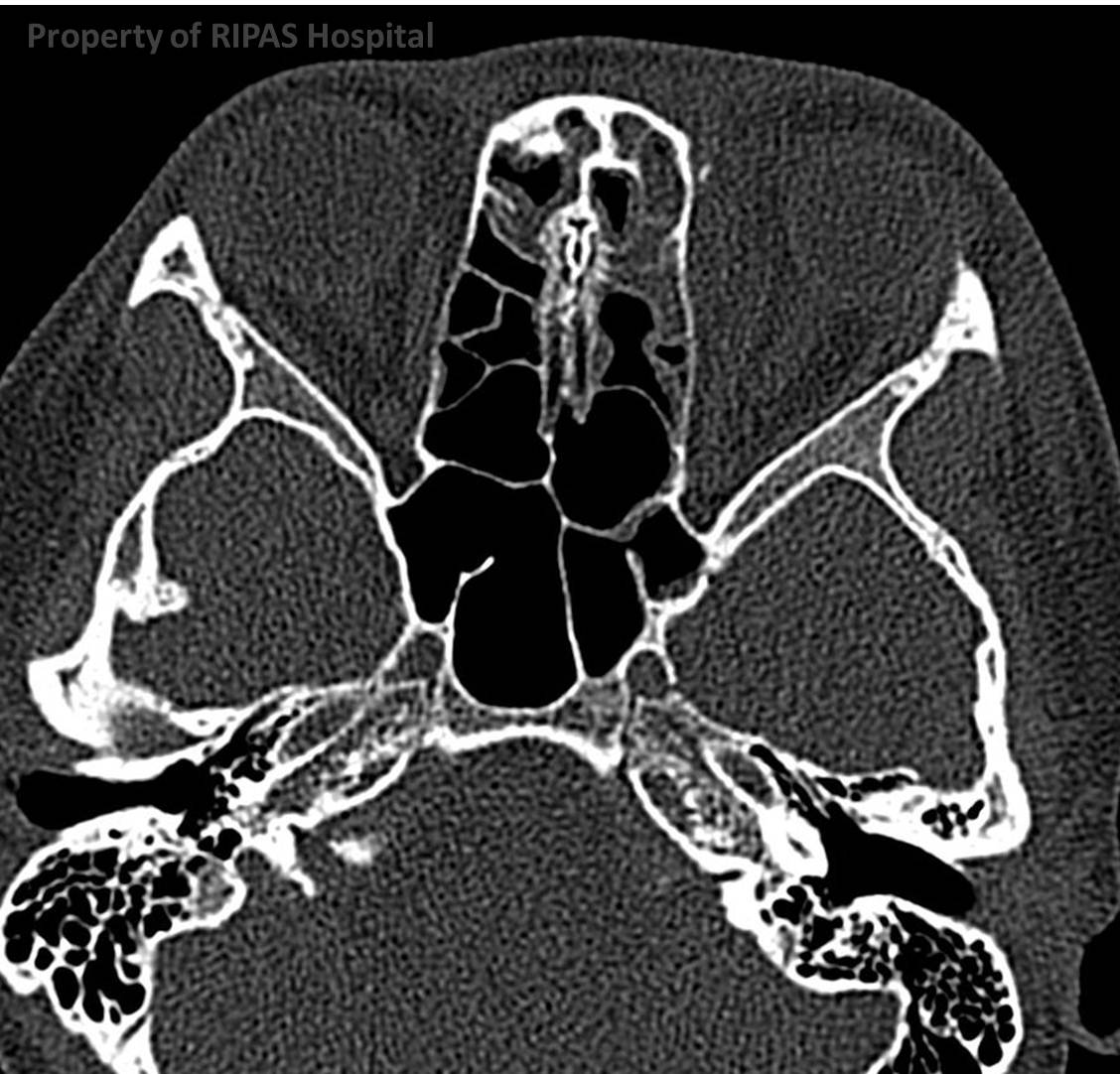
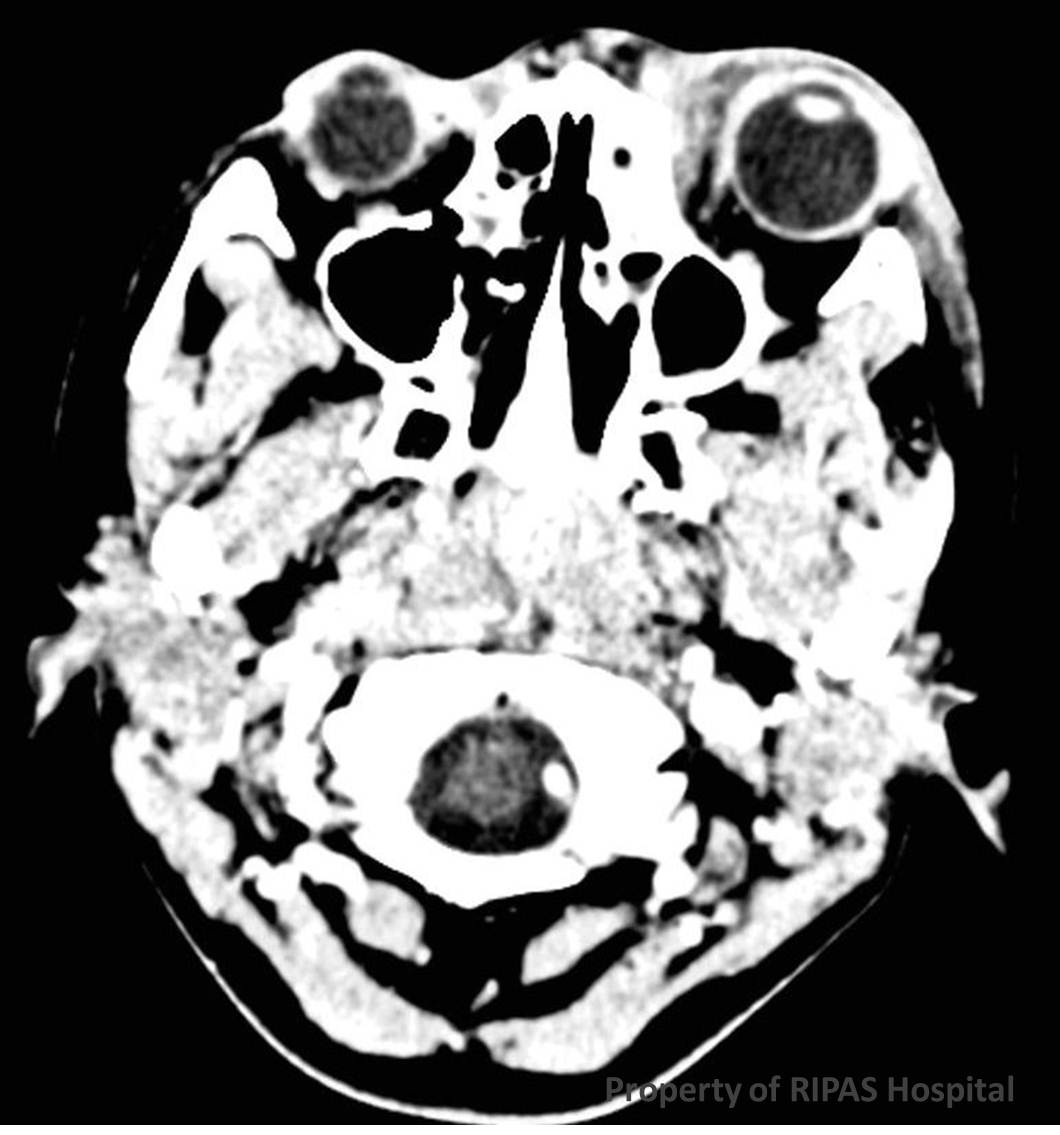
In the acute stage of orbital cellulitis, a CT scan may merely show orbital oedema (Figure 1), but most importantly a subperiosteal abscess (Figure 2). The most common site of a subperiosteal abscess is adjacent to the lamina papyracea of the ethmoid sinuses typically in an elliptical fashion. The collection lies in the extra-conal space. The paranasal sinuses frequently contain sinus disease (Figure 3).
|
|
|
|
|
Figure 2: Click on image to enlarge |
Figure 3: Click on image to enlarge |
|
Orbital cellulitis is typically treated conservatively in the first instance. Intravenous (IV) antibiotics, decongestants and saline irrigation form the mainstay of the conservative treatment. If the clinical condition doesn’t improve within the first 24 to 48 hours patients are usually rescanned.
Further management depends on the CT findings and the clinical situation. Indications for prompt surgery include the deterioration of vision.
Image and text contributed and prepared by
Dr Ian Bickle, Department of Radiology, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()