Figure 1: Click on image to enlarge
IMAGE OF THE WEEK 2012
WEEK 8
DIVERTICULAR DISEASE
|
|
|
|
|
Figure 1: Click on image to enlarge |
|
|
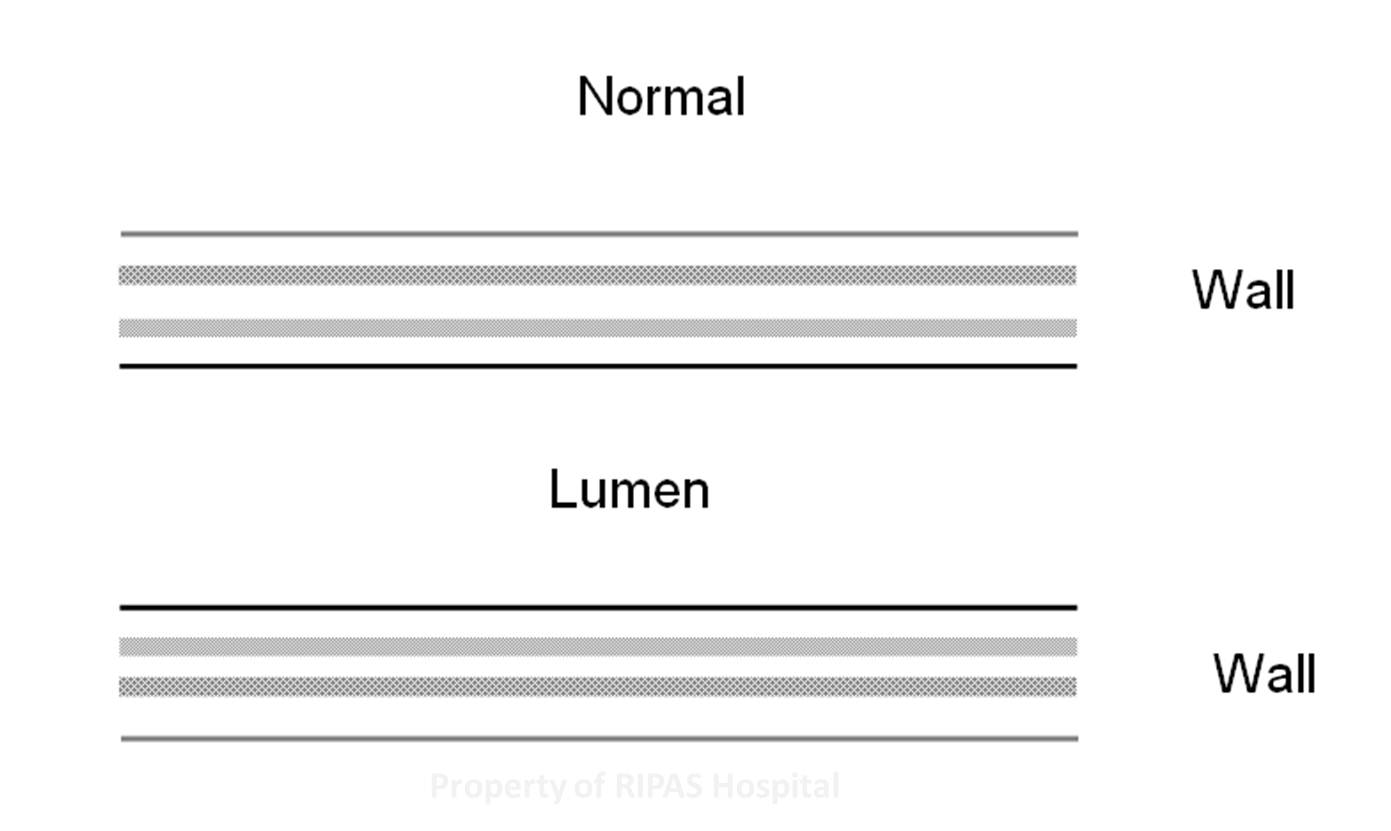
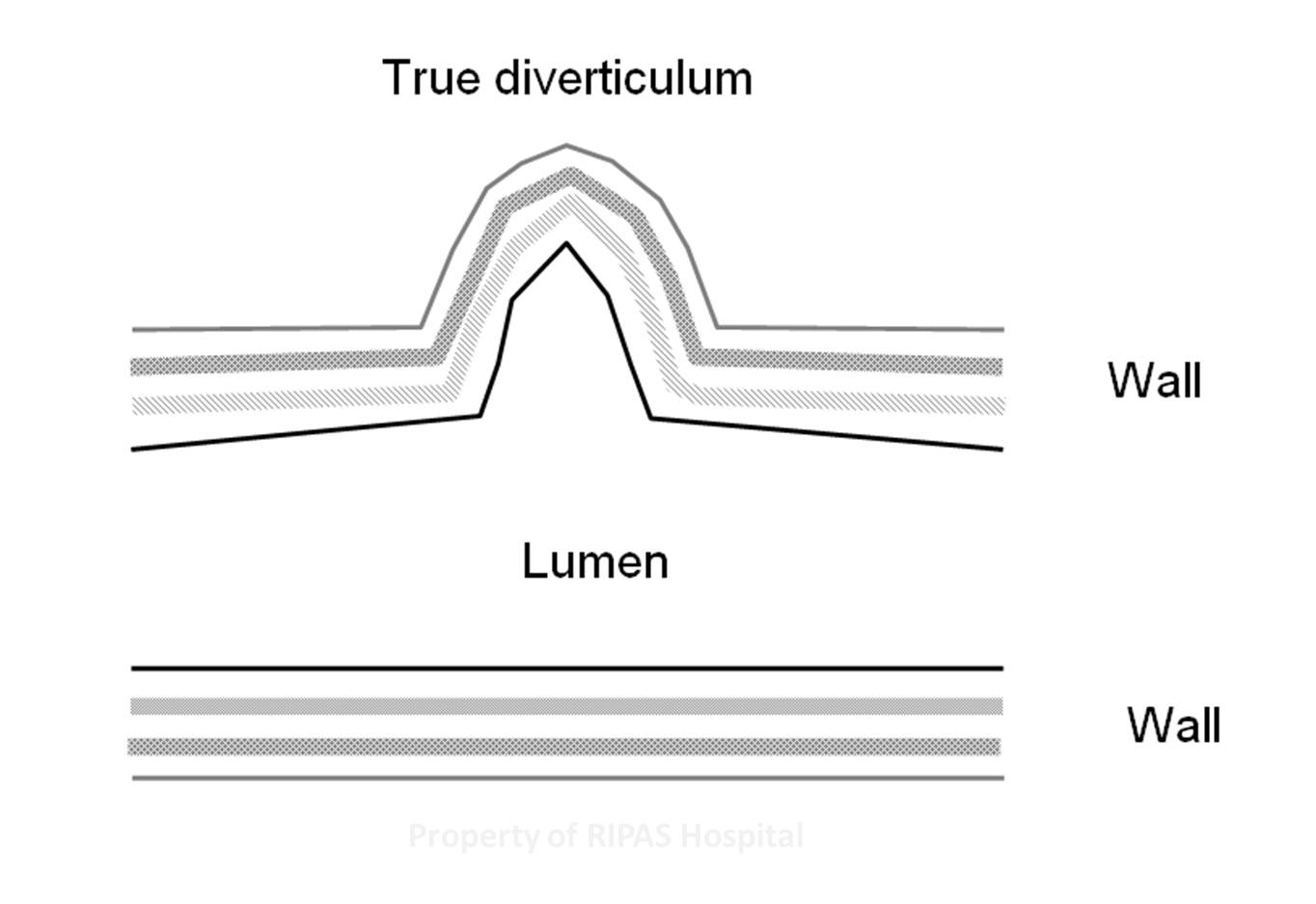
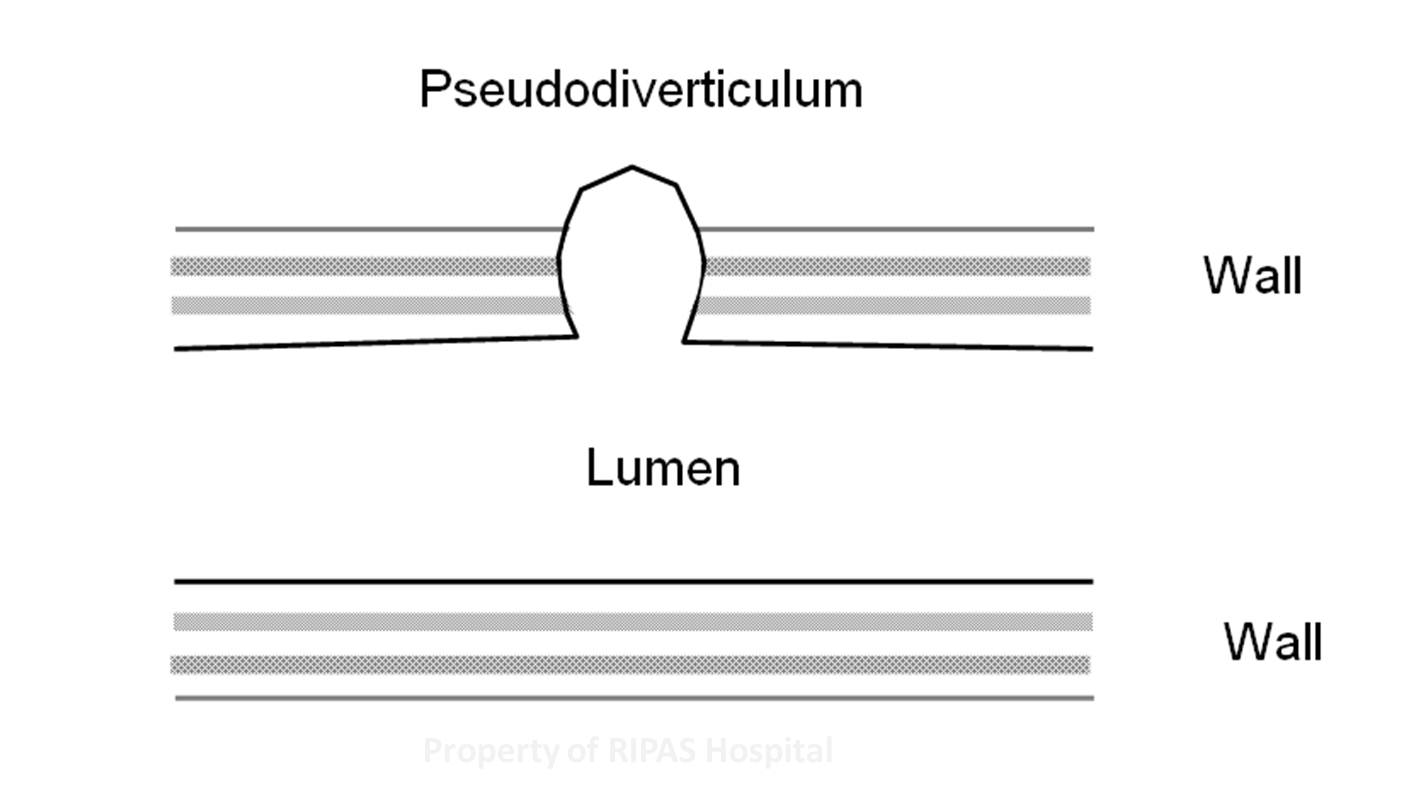
The diverticular seen in diverticular disease is a false diverticulum due to out pouching of the colonic mucosa through the muscle layers where the vessels penetrate through the colon (Figure 1 & Figure 2c). An example of a true divericulum is the Meckel’s diverticulum (rule of 2s: 2 percent of the population, 2 feet away from ileoceacal vale and 2 inches big) found in the ileum (Figure 2b).
|
|
|
 |
|
Figure 2a: Normal Bowel |
Figure 2b: True Diverticulum |
Figure 2c: Pseudodiverticulum |
Diverticular is generally considered a disease of the elderly (50-60% in those aged 80 and above) and is uncommon in those aged 40 or younger (less than 10%). It is more common in the West but the incidence is reported to be increasing in the East. It is most commonly associated with diet lack of fibre. This may explain the rising incidence of diverticular disease in the East. The incidence of diverticular disease is approximately 12.1% (BIMJ 2012; 8 (1) page 27-33) in a Southeast Asian population. There is also variation in the location of diverticular. Left sided diverticular disease (rectum, sigmoid and descending colon) predominates in the West whereas in the East, right sided diverticular disease (ceacal and ascending colon) is more common.
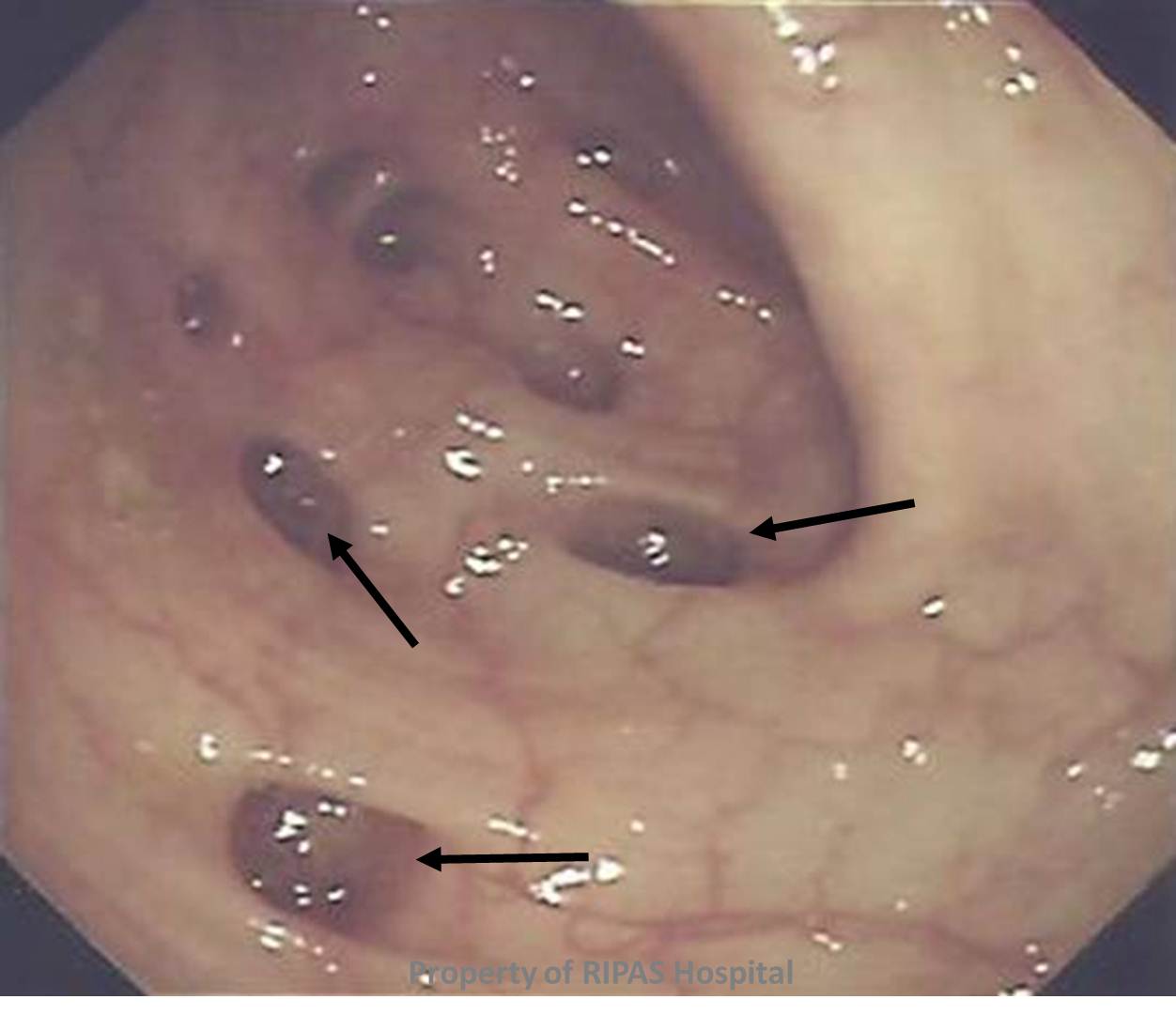
Lack of fibre in the diet leads to delayed stool clearance which are harder in consistency and lead to increased segmentation pressure. The increase in segmentation pressure leads the prolapse of the weakest part of the colonic wall, the points where blood vessels penetrate the colonic wall (arrows in Figure 3) to supply the submucosa and mucosa resulting in formation of pseudodiverticulum. Once the pseudodiverticulum form, it does not regress. Risk factors include increasing age, constipation and connective disease (Marfan’s disease). There is also hereditary predisposition; however, this may be due to shared dietary behaviours.
|
|
|
Figure 3: Diverticulum in large bowel. |
Most patients are not aware of that they have diverticular disease and only a minority is symptomatic. Even for those who have symptoms most are not aware that it is due to diverticular disease as the symptoms are very non specific. Common symptoms include abdominal pain and bloating which are also seen in many gastrointestinal conditions. Diverticular disease is associated with the presence of hiatus hernia and gallstones disease (Saint’s triad).
Serious complications include diverticulitis (due to obstruction of the pseuodiverticulum lumen most commonly feacal material), perforation with diverticular abscess, bleeding, obstruction and fistulation.
Management includes increase in fibre intake to reduce formation of more diverticulum and to reduce the risk of complications. Complicated diverticular disease usually requires surgical treatment by resection of the segment involved. For bleeding diverticular disease, endoscopic or angiographic treatment is also useful.
Image and text contributed and prepared by
Dr Chong Vui Heng, Gastroenterology & Hepatology Unit, Department of Internal Medicine, RIPAS Hospital, Brunei Darussalam.
All images are copyrighted and property of RIPAS Hospital.
![]()