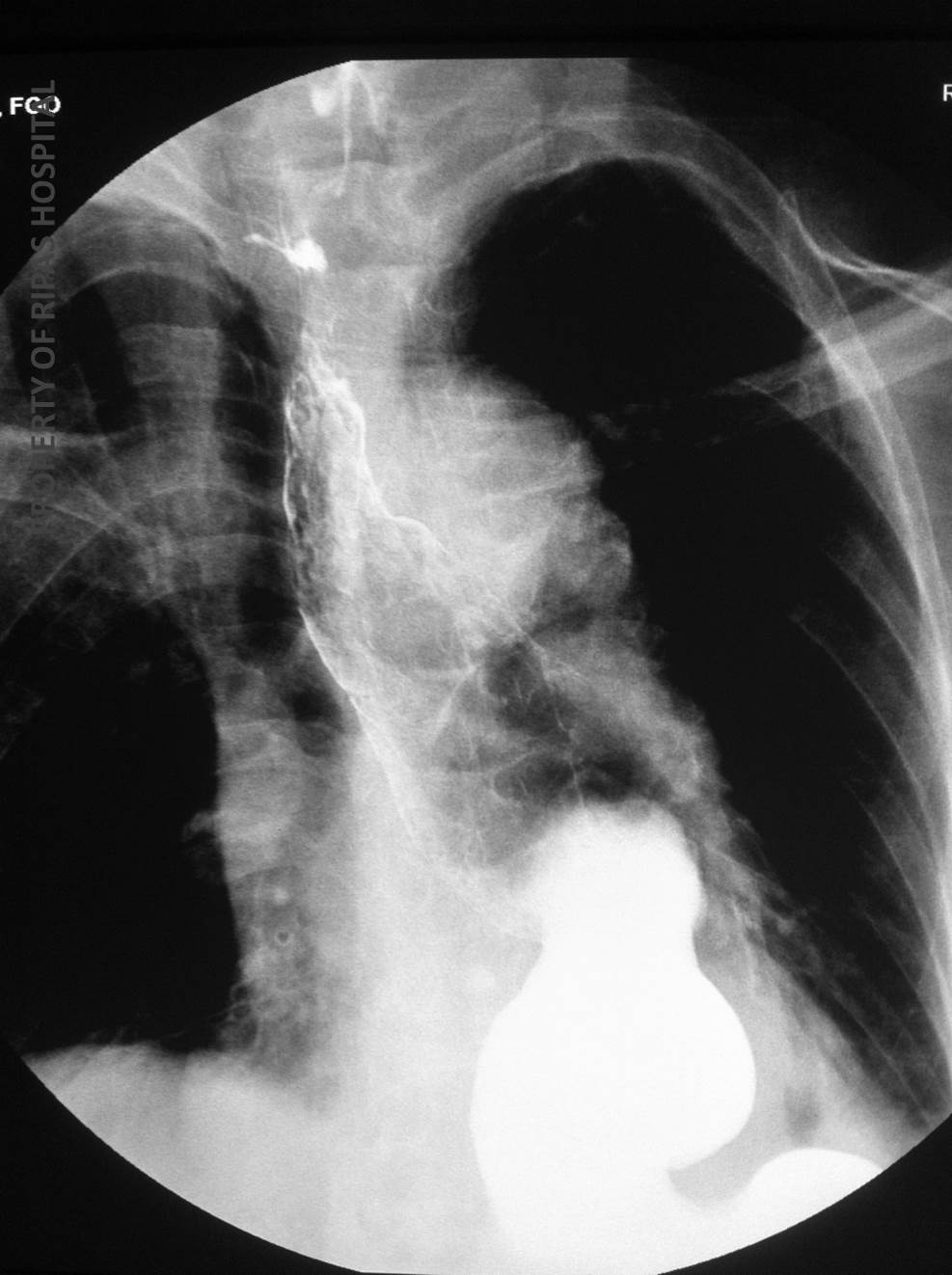
Figure 1: Barium swallow outlining the stomach with an apple core appearance in the middle part of the stomach as indicated by the 2 white arrows.
(Click on image to enlarge)
IMAGE OF THE WEEK 2014
IMAGE 2
GASTRIC CARCINOMA
|
|
|
|
Figure 1: Barium swallow outlining the stomach with an apple core appearance in the middle part of the stomach as indicated by the 2 white arrows. (Click on image to enlarge) |
|
In contemporary medicine radiology is largely confined to staging an endoscopic ally identified tumour and in post treatment surveillance. It rarely has a role in diagnosis, aside from when incidentally identified or on the rare occasion a patient can either not tolerate or is unwilling to undergo an endoscopy.
Therefore a barium meal is uncommonly performed. It may also be undertaken in gastric outlet obstruction or with an individual surgeon’s personal preference prior to surgical planning.
The following features may occur on barium meal:
a. Mucosal irregularity and ulceration
b. Stricturing with irregular shouldering similar to the ‘apple-core’ appearance on barium enema in colorectal carcinoma (Figure 1)
c. Gastric outlet obstruction (Figure 2 & 3)
d. A filling defect in the stomach if large and polypoidal
e. Pseudoachalasia – if the tumour is close to the GO junction and infiltrates the sphincter complex.
f. A non-distensible stomach – with Linitis Plastica.
|
|
|
|
Figure 2: Delay emptying of the stomach with residual contrast due to gastric outlet obstruction by the tumour. (Click on image to enlarge) |
Figure 3: Delay emptying of the stomach with residual contrast due to gastric outlet obstruction by the tumour. (Click on image to enlarge) |
On endoscopy, the appearance of gastric carcinoma or tumour varies from very early subtle looking to very obvious lesions. Early gastric cancer typically appears as a gastritic patch, erosions or ulceration that is flat, depressed or elevated or combination (Refer to Image of the Week 20, 2011). Use of assisted enhanced imaging such as chromoendoscopy with dye (indigo carmine or methylene blue) or electronic chromoendoscopy using different light wavelength (narrow band imaging). Using such imaging provide a clearer distinction between normal and abnormal mucosa. Advanced tumours are typically ulcerated lesions that are friable and also compromise the gastric lumen. Some less early tumour resembles gastric ulcers; hence all gastric ulcer should be biopsied or followed up until healing is documented. A repeat endoscopy is usually done 6-8 weeks with full acid suppression therapy.
Gastric cancers (adenocarcinoma) consist of two major histological type based on the Lauren classification: intestinal type or diffuse type. The intestinal type is often associated with intestinal metaplasia and is often associated with Helicobacter pylori infection. Chronic infection leads to changes from gastritis, atrophy, metaplasia, dysplasia and eventual neoplastic transformation. The diffuse type also refers to as Signet cell carcinoma is typically infiltration and the overlying mucosa may be normal (linitus plastic). The histology is characterised by mucin filled tumour cells with the nuclei displaced periphery given a signet ring features. Less common type of gastric neoplasms/tumour are lymphoma, gastrointestinal stromal tumour (GIST) and neuroendocrine tumour.
Helicobacter pylori is the most common aetiological agent. Unknown to many, Epstein Barr Virus (EBV) is the second most common infection associated with gastric cancer (~10%).
In Brunei Darussalam, Gastric cancer is the second most common gastrointestinal cancer after colorectal cancer. Each year, there are approximately between 25-30 cases recorded and the trend is increasing. Most are diagnosed at moderate to advanced stages.
Treatment (partial or total gastrectomy) is curative resection if possible. Chemotherapy may be required depending on the surgical findings. Helicobacter pylori if present needs to be eradication.
Images and text contributed by
Dr Ian Bickle, Department of Radiology,RIPAS Hospital
and
Dr Chong Vui Heng, Department of Internal Medicine, RIPAS Hospital
All images are copyrighted and property of RIPAS Hospital.
![]()